📋 Table of Contents
- → Introduction
- → The Joe Tippens Connection
- → NSCLC vs SCLC: Why It Matters
- → Mechanisms of Action in Lung Cancer
- → NSCLC Research: The 2018 Yale Study
- → SCLC Evidence and Limitations
- → FBZ + DADA: Synergistic Combination
- → Dosage and Protocols
- → Safety and Side Effects
- → Interaction with Lung Cancer Chemotherapy
- → Frequently Asked Questions
- → Clinical Evidence & Limitations
- → References
Shop Sanare Lab
Below are commonly referenced items. Links are provided for convenience — always review the label and consult a professional before use.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
6 / 12 / 18 mg — 100 tablets
120 capsules — with Black Pepper for absorption
Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.
Lung cancer remains the leading cause of cancer-related deaths worldwide, accounting for approximately 1.8 million deaths annually. For patients facing this diagnosis — particularly those with aggressive subtypes like small cell lung cancer (SCLC) or advanced non-small cell lung cancer (NSCLC) — the search for additional therapeutic options can feel urgent and deeply personal.
Fenbendazole (FBZ) first entered public consciousness through the story of Joe Tippens, who reported achieving remission from stage IV SCLC while using a self-directed protocol that included this veterinary antiparasitic drug. His story sparked a wave of interest in fenbendazole as a potential anticancer agent, leading researchers to investigate its mechanisms and efficacy in preclinical lung cancer models.
This article examines the scientific evidence for fenbendazole in lung cancer — from the foundational 2018 Yale study documenting its activity in NSCLC cell lines, to recent 2025 research on synergistic combinations, to the critical limitations that prevent clinical recommendations. We cover mechanism of action, dosing considerations, safety profiles, and the key distinction between NSCLC and SCLC subtypes that every patient should understand.
⚠️ Medical Disclaimer
This article is for research and informational purposes only. It does not constitute medical advice and is not a substitute for professional oncology consultation. Always discuss any investigational protocol with your physician.
Why Lung Cancer and Fenbendazole?
Lung cancer is broadly classified into two main types: non-small cell lung cancer (NSCLC), which accounts for approximately 85% of cases, and small cell lung cancer (SCLC), which represents about 10-15% but is notably more aggressive. Both types present significant treatment challenges:
- NSCLC: While targeted therapies (EGFR inhibitors, ALK inhibitors) and immunotherapy (pembrolizumab, nivolumab) have improved outcomes for specific subtypes, many patients eventually develop resistance. Five-year survival for metastatic NSCLC remains around 7%.
- SCLC: This highly aggressive subtype typically presents with metastatic disease at diagnosis. Standard treatment includes platinum-based chemotherapy (cisplatin or carboplatin) plus etoposide, but relapse is common and prognosis is poor — median survival for extensive-stage SCLC is 8-13 months.
Fenbendazole's potential relevance to lung cancer stems from several converging factors: Joe Tippens' SCLC diagnosis and reported remission, preclinical research documenting activity in NSCLC cell lines, and mechanistic rationale suggesting it may target pathways relevant to both subtypes.
🧑 The Joe Tippens Connection: SCLC and the Original Story
In 2016, Joe Tippens was diagnosed with small cell lung cancer with metastatic disease. SCLC is characterized by rapid growth, early metastasis, and historically poor outcomes even with aggressive treatment. Joe began standard-of-care platinum-based chemotherapy but reported severe esophageal complications that made continuation extremely difficult.
During this period, Joe learned about fenbendazole through a veterinary connection and decided to add it to a supplement regimen that included vitamin E (tocotrienols), curcumin with piperine, and CBD oil. Over the following months, his scans reportedly showed significant tumor regression, eventually achieving no evidence of disease (NED).
Critical Context: Joe's case is a single anecdotal report. He was receiving conventional treatment during this period, making it impossible to isolate fenbendazole's contribution to his outcome. His story is not clinical proof, but it sparked scientific interest and drove preclinical research into fenbendazole's mechanisms in lung cancer models.
For a comprehensive overview of the Joe Tippens protocol, see: Joe Tippens Protocol.
🔬 NSCLC vs SCLC: Why the Distinction Matters
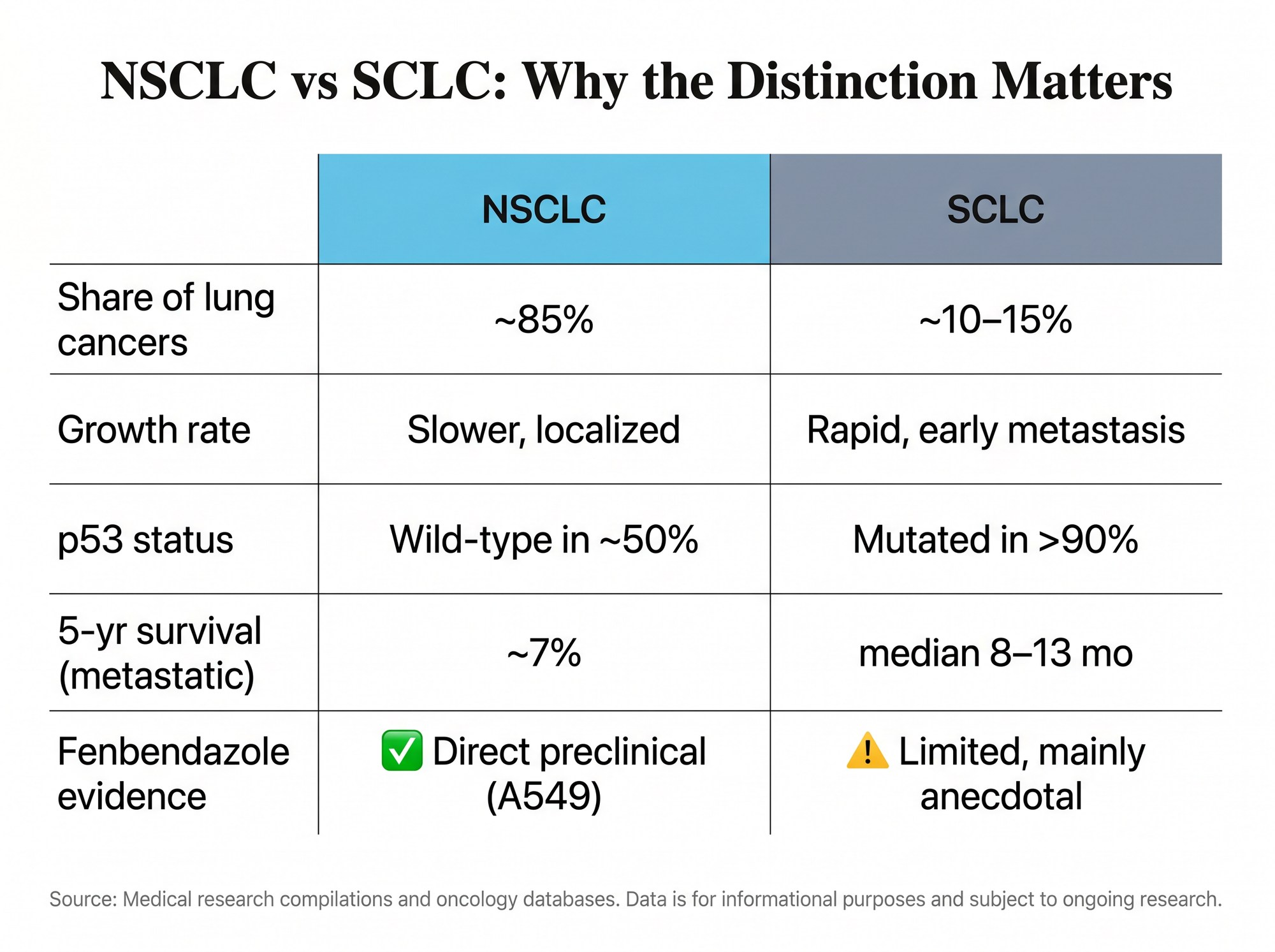
Understanding the biological differences between NSCLC and SCLC is critical when evaluating fenbendazole's potential relevance:
| Feature | NSCLC (Non-Small Cell) | SCLC (Small Cell) |
|---|---|---|
| Prevalence | ~85% of lung cancers | ~10-15% of lung cancers |
| Growth rate | Slower, more localized initially | Extremely rapid, early metastasis |
| Histology | Adenocarcinoma, squamous, large cell | Neuroendocrine origin, small cells |
| Standard treatment | Surgery (early), targeted therapy, immunotherapy, chemotherapy | Chemotherapy (cisplatin + etoposide), radiation |
| Targeted therapy | EGFR, ALK, ROS1, BRAF, MET inhibitors available | Limited targeted options; immunotherapy emerging |
| Prognosis (metastatic) | 5-year survival ~7% | Median survival 8-13 months (extensive stage) |
| Fenbendazole research | ✅ Direct preclinical evidence (2018 Yale study, A549 cells) | ⚠️ Limited preclinical data; mainly anecdotal (Joe Tippens) |
Key Takeaway: Most rigorous preclinical research on fenbendazole has been conducted using NSCLC cell lines (particularly A549 adenocarcinoma cells). Direct evidence for SCLC is far more limited, despite Joe Tippens' SCLC diagnosis driving public interest.
🧬 Mechanisms of Action: How Fenbendazole Affects Lung Cancer Cells
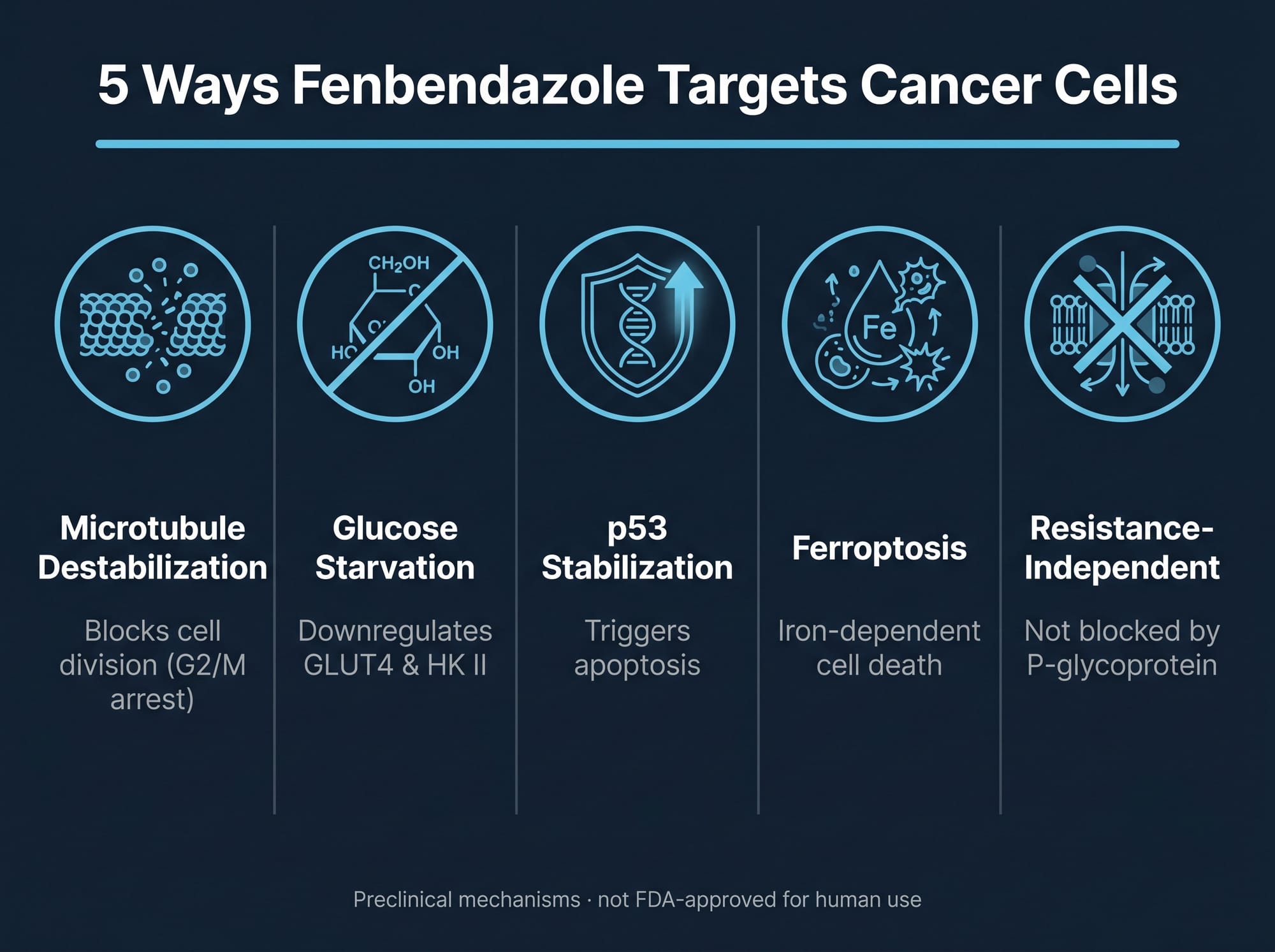
Preclinical research has identified several distinct mechanisms through which fenbendazole may affect lung cancer cells. Understanding these pathways helps explain both its potential and its limitations.
1. Microtubule Destabilization
Fenbendazole belongs to the benzimidazole class of compounds, which are known microtubule-targeting agents. The 2018 study published in Scientific Reports (Nature) by Dogra, Kumar, and Mukhopadhyay from MD Anderson Cancer Center demonstrated that fenbendazole acts as a moderate microtubule-destabilizing agent in A549 human NSCLC cells (PMC6103891).
Mechanism:
- Fenbendazole binds to β-tubulin at the colchicine-binding site
- Disrupts microtubule polymerization — the process by which tubulin proteins assemble into structural microtubules
- Prevents proper formation of the mitotic spindle during cell division
- Leads to G2/M cell cycle arrest — cancer cells stall at the transition from DNA replication (G2 phase) to mitosis (M phase)
- Triggers mitotic catastrophe and apoptosis (programmed cell death)
Clinical Context: This is the same general mechanism exploited by established chemotherapy drugs like paclitaxel (Taxol), vincristine, and vinblastine. For more details, see our guide on Joe Tippens Protocol. However, unlike taxanes that stabilize microtubules, fenbendazole destabilizes them.
2. Glucose Metabolism Disruption (GLUT Inhibition)
Cancer cells exhibit a phenomenon known as the Warburg effect — they consume glucose at rates 10-100 times higher than normal cells, even in the presence of oxygen, relying on glycolysis for energy production. The 2018 MD Anderson study demonstrated that fenbendazole inhibits glucose uptake in A549 lung cancer cells.
Mechanism:
- Downregulates expression of GLUT4 (glucose transporter type 4)
- Reduces hexokinase II (HK II) expression — the enzyme that catalyzes the first committed step of glycolysis
- Effectively "starves" cancer cells by cutting off their primary energy source
- This metabolic interference is distinct from microtubule disruption, representing a second independent pathway
Significance: This mechanism is particularly relevant because standard chemotherapy drugs do not typically target glucose metabolism. Fenbendazole's dual action (microtubules + metabolism) creates convergent pressure on cancer cells from two different angles.
3. p53 Stabilization and Mitochondrial Translocation
The tumor suppressor protein p53 is often called the "guardian of the genome" because it prevents cells with damaged DNA from dividing. The 2018 study documented that fenbendazole induces mitochondrial translocation of p53 in NSCLC cells.
Mechanism:
- Fenbendazole stabilizes p53 protein levels
- Downregulates Mdm2 and MdmX — proteins that normally inhibit p53 function
- Promotes p53 translocation to mitochondria, where it triggers intrinsic apoptotic pathways
- Activates pro-apoptotic Bcl-2 family proteins (Bax, Bak)
- Results in mitochondrial outer membrane permeabilization (MOMP) and caspase-mediated apoptosis
Clinical Relevance: Approximately 50% of human cancers harbor p53 mutations. In cancers with wild-type (functional) p53, agents that stabilize p53 can restore its tumor-suppressive function. However, in p53-mutant cancers, this mechanism may be less effective.
4. Ferroptosis Induction (Emerging Research)
Recent research suggests fenbendazole may trigger ferroptosis — an iron-dependent form of non-apoptotic cell death characterized by lipid peroxidation. This mechanism is particularly relevant in cancers resistant to apoptosis.
Mechanism:
- Induces reactive oxygen species (ROS) accumulation
- Causes lipid peroxidation in cancer cell membranes
- Iron-dependent process distinct from apoptosis, necroptosis, or autophagy
- May remain active in apoptosis-resistant cancer cells
5. Drug Resistance Profile: P-glycoprotein Independence
A critical finding from the 2018 study: fenbendazole is neither a substrate nor an inhibitor of P-glycoprotein (P-gp). P-gp is a drug efflux pump that cancer cells often overexpress to pump chemotherapy drugs out of cells, creating multidrug resistance (MDR).
Significance: Because fenbendazole does not rely on P-gp for cellular entry or exit (unlike some other antiparasitics — see Fenbendazole vs Ivermectin), it may retain activity in cancer cells that have developed resistance to other microtubule-targeting drugs like paclitaxel or vinblastine.
🔬 NSCLC Research: The 2018 Yale/MD Anderson Study
The most directly relevant preclinical study on fenbendazole in lung cancer is the 2018 paper published in Scientific Reports by Dogra, Kumar, and Mukhopadhyay from MD Anderson Cancer Center (PMC6103891). This study used A549 human NSCLC cells — one of the most widely used lung adenocarcinoma cell lines in cancer research.
Key Findings:
| Parameter | Finding |
|---|---|
| Cell line | A549 (human lung adenocarcinoma, NSCLC) |
| IC₅₀ (72h) | ~100 nM (nanomolar) in vitro |
| Mechanism | Moderate microtubule destabilization + glucose uptake inhibition + p53 stabilization |
| Cell cycle effect | G2/M arrest |
| Apoptosis markers | Increased cleaved caspase-3, PARP cleavage |
| GLUT4 expression | Significantly reduced |
| HK II expression | Significantly reduced |
| p53 mitochondrial translocation | Confirmed by Western blot and immunofluorescence |
| P-gp interaction | No substrate/inhibitor activity (resistance-independent) |
In Vivo (Animal) Data: The study did not include xenograft tumor models in mice, limiting conclusions about in vivo efficacy, bioavailability, and pharmacokinetics. This is a significant gap in the evidence base.
Interpretation: This study provides proof-of-concept that fenbendazole has anticancer activity in NSCLC cell lines through multiple independent mechanisms. However, cell culture efficacy does not guarantee clinical benefit in humans.
⚠️ SCLC Evidence and Limitations
Despite Joe Tippens' SCLC diagnosis driving public interest, direct preclinical research on fenbendazole in SCLC models is notably limited. Learn more about fenbendazole dosage guide.
What We Don't Know About FBZ and SCLC:
- No published studies using SCLC cell lines (e.g., H69, H146, DMS-114) to test fenbendazole's activity
- No xenograft studies in SCLC tumor-bearing mice
- No data on fenbendazole's interaction with standard SCLC chemotherapy (cisplatin + etoposide)
- No pharmacokinetic studies in SCLC models
Biological Differences That May Matter:
| Feature | NSCLC | SCLC |
|---|---|---|
| Growth rate | Moderate | Extremely rapid (doubling time ~30 days) |
| p53 status | Wild-type in ~50% | Mutated/deleted in >90% (TP53 + RB1 co-mutation) |
| Metabolism | Glycolysis-dependent (Warburg effect) | Also highly glycolytic + neuroendocrine features |
| Microtubule dynamics | Standard mitotic machinery | Rapid mitotic activity, high proliferation index |
| Drug sensitivity | Variable; resistance develops over time | Initially chemosensitive, but rapid relapse with resistance |
Key Concern: SCLC typically has mutated or deleted p53 (via TP53 loss) and RB1 inactivation. Because fenbendazole's p53-stabilization mechanism relies on functional p53, this pathway may be non-operational in SCLC. However, the microtubule disruption and glucose metabolism mechanisms are p53-independent and may still be relevant.
Bottom Line: Extrapolating NSCLC cell line data to SCLC is biologically questionable without direct experimental validation. The anecdotal success of Joe Tippens does not substitute for rigorous preclinical testing in SCLC models.
For other metabolic combination approaches, see the ISOM Protocol and the Care Oncology Protocol (COC), which use repurposed drugs targeting similar metabolic pathways.
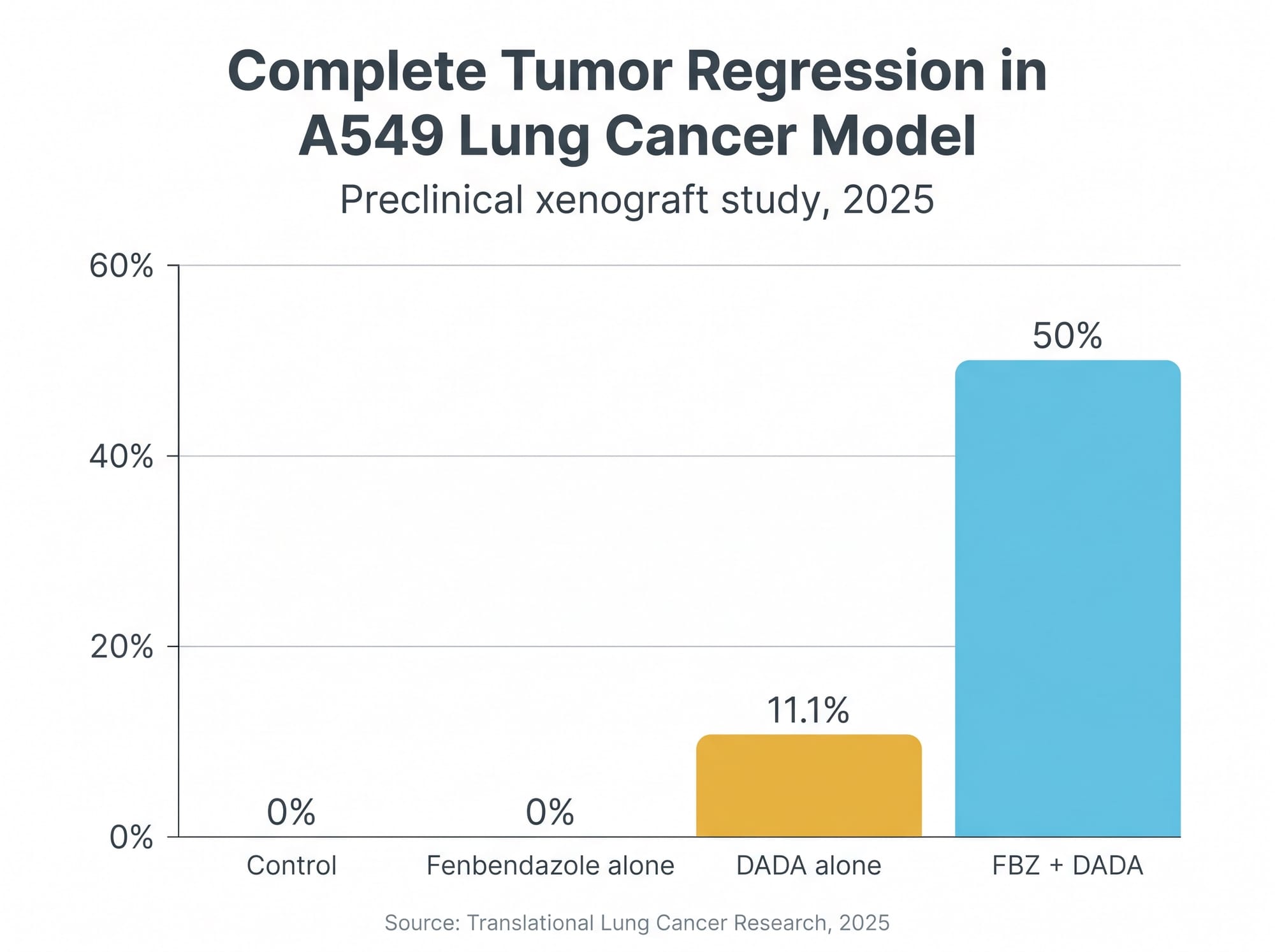
💡 FBZ + DADA: Synergistic Combination for Enhanced Efficacy and Safety
One of the most recent developments in fenbendazole lung cancer research is the investigation of diisopropylamine dichloroacetate (DADA) as a combination partner. A 2025 study published in Translational Lung Cancer Research explored this combination in A549 NSCLC xenograft models (TLCR 2025).
Rationale for the Combination:
Problem: Fenbendazole use has been associated with drug-induced liver injury (DILI) in some case reports and self-administration scenarios. This hepatotoxicity risk limits long-term use and higher dosing.
Solution: DADA is a derivative of dichloroacetate (DCA), a compound with known metabolic anticancer activity and hepatoprotective properties. Combining fenbendazole with DADA aims to:
- Enhance antitumor efficacy through synergistic metabolic disruption
- Reduce hepatotoxicity risk
- Allow more sustained treatment without liver damage
Study Design and Results:
Model: Immunodeficient BALB/c nude mice transplanted with A549 human lung cancer cells (subcutaneous xenografts)
Treatment Groups:
| Group | Dose | Complete Tumor Regression Rate |
|---|---|---|
| Control | Vehicle only | 0% |
| Fenbendazole alone | 40 mg/kg daily | 0% |
| DADA alone | 100 mg/kg daily | 11.1% |
| FBZ + DADA | 40 mg/kg FBZ + 100 mg/kg DADA | 50% ✅ |
Key Findings:
- The combination produced 50% complete tumor regression — tumors disappeared entirely and did not recur during the study period
- Fenbendazole alone at this dose did not produce any complete regressions
- The combination was synergistic, not merely additive
- Safety profile was improved: No significant body weight loss, no elevation in liver enzymes (ALT/AST), no kidney function impairment, normal blood glucose
- Mice tolerated the combination well with no observable toxicity
Mechanistic Explanation:
- Fenbendazole: Microtubule disruption + GLUT4/HK II inhibition (blocks glucose uptake and glycolysis entry)
- DADA: Inhibits pyruvate dehydrogenase kinase (PDK), forcing cancer cells to shift from glycolysis to oxidative phosphorylation, which they cannot sustain as effectively
- Convergent metabolic pressure: Fenbendazole blocks glucose entry, DADA blocks glycolytic metabolism — cancer cells are metabolically "trapped"
Clinical Implications: This combination represents a potential strategy to improve fenbendazole's efficacy while mitigating hepatotoxicity concerns. However, DADA is not commercially available, and this remains a preclinical proof-of-concept that has not been tested in humans.
💊 Dosage and Protocols for Lung Cancer
Because fenbendazole is not FDA-approved for human use and no clinical trials have established human dosing for lung cancer, all dosing information is empirical and anecdotal, derived from the Joe Tippens protocol and online patient communities.
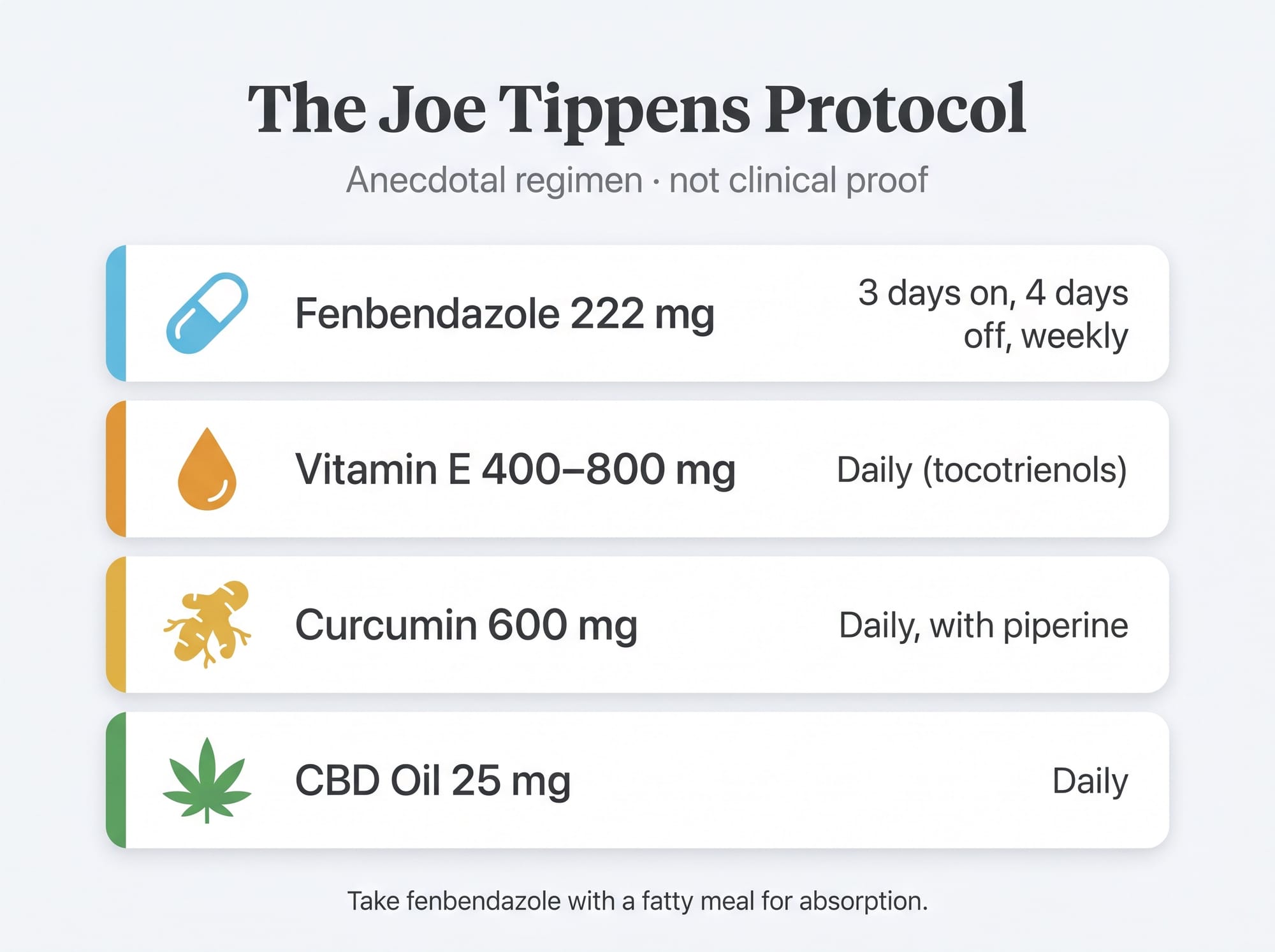
Standard Fenbendazole Dosing (Joe Tippens Protocol):
| Component | Dosage | Schedule | Administration |
|---|---|---|---|
| Fenbendazole | 222 mg | Daily for 3 days, then 4 days off (repeat weekly) | With fatty meal (yogurt, peanut butter, avocado) for absorption |
| Vitamin E | 400-800 mg | Daily (tocotrienols preferred) | With meals |
| Curcumin | 600 mg | Daily (two 300 mg doses) | With black pepper (piperine) for bioavailability |
| CBD Oil | 25 mg | Daily | Full or broad-spectrum |
Alternative/Modified Schedules Discussed Online:
- Continuous dosing: 222 mg daily, 7 days/week (no scheduled breaks)
- Higher dose: 444 mg daily (double dose) for more aggressive disease
- 6-on/1-off: Daily for 6 days, 1 day off per week
Important Notes:
- None of these dosing schedules have been validated in clinical trials
- The original 222 mg dose is based on veterinary antiparasitic dosing, not cancer pharmacokinetics
- Optimal human dosing for anticancer activity is unknown
- Fenbendazole is lipophilic — taking it with dietary fat significantly improves absorption
Panacur C vs. Pharmaceutical-Grade Capsules:
| Product | Pros | Cons |
|---|---|---|
| Panacur C Granules | Widely available, low cost, Joe Tippens used this | Veterinary formulation, contains additives/flavorings, requires measuring (1g ≈ 222mg FBZ) |
| Pharmaceutical-grade capsules | Precise dosing (222mg, 444mg), third-party lab tested, no veterinary additives | Higher cost, fewer brands available |
For detailed dosing guidance and safety considerations, see: Fenbendazole Dosage Guide. Learn more about fenbendazole and breast cancer.
⚠️ Safety and Side Effects in Lung Cancer Context
While fenbendazole has a wide safety margin in veterinary use, human safety for long-term cancer treatment is not well-established. Reported side effects and safety concerns include:
Common Side Effects (Mild to Moderate):
- Gastrointestinal disturbances: Nausea, diarrhea, abdominal discomfort, gas (most frequently reported in online communities)
- Fatigue: Mild fatigue or "brain fog" during initial use, often resolving after the first few weeks
- Headache: Occasionally reported, typically mild
Management: Taking fenbendazole with food (especially fatty food) often reduces GI symptoms.
Serious Side Effects (Rare but Documented):
1. Hepatotoxicity (Liver Injury):
The most serious documented risk. Case reports of drug-induced liver injury (DILI) associated with fenbendazole use exist in medical literature. For a detailed analysis, see Fenbendazole and Liver Safety.
Manifestations:
- Elevated ALT, AST (liver enzymes)
- Elevated alkaline phosphatase
- Elevated bilirubin (jaundice in severe cases)
- Abdominal pain, nausea, dark urine
Monitoring:
- Baseline liver function tests (LFTs) before starting fenbendazole
- Periodic monitoring: Every 4-6 weeks during use
- Stop fenbendazole immediately if ALT/AST >3× upper limit of normal (ULN)
- Consult physician for evaluation if liver enzyme elevation occurs
2. Bone Marrow Suppression:
Neutropenia (low white blood cell count) has been reported in rare cases, particularly with prolonged high-dose use.
Concern for Lung Cancer Patients: Many lung cancer chemotherapy regimens (cisplatin, etoposide, docetaxel) already cause myelosuppression. Adding fenbendazole could theoretically create additive bone marrow effects.
Monitoring:
- Complete blood count (CBC) at baseline and periodically during use
- Watch for signs of infection (fever, chills), unusual bruising, or bleeding
- Coordinate monitoring with oncologist if using fenbendazole alongside chemotherapy
Contraindications:
- Pregnancy and breastfeeding: Fenbendazole is teratogenic (causes birth defects) in animal studies — do not use during pregnancy or breastfeeding
- Pre-existing liver disease: Patients with hepatitis, cirrhosis, or other liver conditions should exercise extreme caution or avoid fenbendazole entirely
- Hypersensitivity to benzimidazoles: Avoid if allergic to mebendazole, albendazole, or other benzimidazole drugs
🩺 Interaction with Lung Cancer Chemotherapy
One of the most urgent questions lung cancer patients ask: "Can I use fenbendazole while I'm on chemotherapy?"
Relevant Preclinical Data: FBZ + Docetaxel
The most directly relevant study is a 2013 paper published in Anticancer Research by Duan, Liu, and Rockwell from Yale University (PMC3580766). The researchers evaluated fenbendazole combined with docetaxel (Taxotere), a chemotherapy drug used in NSCLC, using the EMT6 mouse mammary tumor model.
Key Findings:
- Additive cytotoxicity — no antagonism: Isobologram analysis confirmed that FBZ and docetaxel produced additive effects. Critically, FBZ did not blunt or interfere with docetaxel's anticancer activity.
- No additional toxicity: In mice, FBZ at 50 mg/kg/day caused no additional toxicity beyond docetaxel alone — no weight loss, no behavioral changes, no measurable health impact.
- No synergy observed: The combination did not exceed additivity (no synergy). Both FBZ and docetaxel target microtubules but via opposite mechanisms (FBZ destabilizes, docetaxel stabilizes).
Interpretation: This study suggests FBZ can be safely combined with docetaxel without reducing chemotherapy efficacy or adding toxicity — at least in preclinical models. However, this is one study, one chemotherapy drug, and one cancer type. For data on other cancer types, see our reviews of breast cancer, colorectal & pancreatic cancer, and brain cancer.
Drug Metabolism Interactions: CYP450 Enzymes
A critical concern when combining any supplements with chemotherapy is drug-drug interactions via the cytochrome P450 (CYP) enzyme system.
Fenbendazole: A 2023 study demonstrated that fenbendazole induced CYP1A enzymes in pig liver (19-fold increase in CYP1A1, 14-fold in CYP1A2) (PMID 38141570). Learn more about fenbendazole and prostate cancer.
Concern for Lung Cancer Patients:
- Erlotinib, gefitinib (EGFR inhibitors used in NSCLC) are metabolized by CYP1A2
- CYP1A2 induction by fenbendazole could theoretically reduce plasma levels of these targeted therapies, potentially reducing efficacy
- Always disclose fenbendazole use to your oncologist so drug levels can be monitored if warranted
Practical Recommendations for Concurrent Use:
1. Disclose to Your Oncologist
Full transparency is non-negotiable. Your oncologist cannot monitor for interactions or interpret unusual labs without knowing what supplements you are taking.
2. Monitor Liver Function
Many chemotherapy agents (cisplatin, carboplatin, docetaxel) are hepatotoxic. Adding fenbendazole increases theoretical hepatic load. Check baseline ALT, AST, bilirubin before starting FBZ, then monitor at each chemotherapy cycle.
3. Monitor Blood Counts
Chemotherapy causes myelosuppression. While FBZ is not strongly associated with myelosuppression at standard doses, additive effects are theoretically possible. Maintain standard CBC monitoring.
4. Consider Timing Strategies
| Timing Approach | Rationale | Interaction Risk |
|---|---|---|
| Before chemotherapy | "Prepare" tumor microenvironment 2-4 weeks before chemo | DDI risk from day one of chemo |
| During chemotherapy | Maintain metabolic pressure during chemo; leverage additive effects | Highest risk; requires close monitoring |
| After chemotherapy | Target residual cancer cells, cancer stem cells, micrometastatic disease post-treatment | Lowest DDI risk; no active chemo interaction |
The after-chemotherapy maintenance approach carries the lowest drug-drug interaction risk and may be the most prudent choice for patients concerned about interactions.
For a comprehensive analysis of FBZ-chemotherapy interactions, see: Fenbendazole and Chemotherapy: Can They Be Combined Safely?
Products Referenced in This Research
Lab-tested fenbendazole discussed in the research above — with full certificates of analysis.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
Disclaimer: For convenience only. Consult a licensed professional.
Frequently Asked Questions (FAQ)
❓ 1. Does fenbendazole work for lung cancer?
Answer: Preclinical studies (cell culture and animal models) show fenbendazole has anticancer activity in NSCLC through microtubule disruption, glucose metabolism inhibition, and p53 stabilization. However, there are no completed human clinical trials proving it works in lung cancer patients. The evidence base consists of laboratory research and anecdotal reports (notably Joe Tippens' SCLC story). It should not be used as a substitute for conventional treatment without medical supervision.
❓ 2. What's the difference between NSCLC and SCLC, and does it matter for fenbendazole?
Answer: NSCLC (non-small cell lung cancer) accounts for ~85% of lung cancers and grows more slowly. For more details, see our guide on fenbendazole case reports showing remission. SCLC (small cell lung cancer) accounts for ~10-15% and is extremely aggressive. Most rigorous fenbendazole research has been conducted using NSCLC cell lines (A549). Direct evidence for SCLC is far more limited, despite Joe Tippens' SCLC diagnosis driving public interest. Additionally, SCLC typically has mutated/deleted p53, which may limit the effectiveness of fenbendazole's p53-stabilization mechanism.
❓ 3. Can I use fenbendazole while on chemotherapy for lung cancer?
Answer: Possibly, but only with oncologist knowledge and supervision. Preclinical data (FBZ + docetaxel study) suggest fenbendazole does not interfere with chemotherapy efficacy and may be safely combined. However, drug interactions via CYP450 enzymes are a concern, especially with targeted therapies like erlotinib or gefitinib (EGFR inhibitors). Full disclosure to your oncologist is non-negotiable. See: Fenbendazole and Chemotherapy.
❓ 4. What is the Joe Tippens protocol for lung cancer?
Answer: The Joe Tippens protocol consists of: Fenbendazole 222 mg daily for 3 days, then 4 days off (repeat weekly); Vitamin E 400-800 mg daily (tocotrienols); Curcumin 600 mg daily (with piperine); CBD Oil 25 mg daily. Joe Tippens reported achieving remission from stage IV SCLC while using this protocol alongside conventional treatment. His case is a single anecdotal report and does not constitute clinical proof. For full details, see: Joe Tippens Protocol.
❓ 5. How much fenbendazole should I take for lung cancer?
Answer: There is no established human dosing for lung cancer, as fenbendazole is not FDA-approved for this use. The Joe Tippens protocol uses 222 mg daily for 3 days, then 4 days off. Some users report using 444 mg daily or continuous daily dosing. Optimal human dosing for anticancer activity is unknown. Fenbendazole should be taken with a fatty meal (yogurt, peanut butter, avocado) to improve absorption. See: Fenbendazole Dosage Guide.
❓ 6. What are the side effects of fenbendazole for lung cancer?
Answer: The most common side effects are mild gastrointestinal symptoms: nausea, diarrhea, abdominal discomfort, gas. These often resolve after the first few weeks or can be reduced by taking fenbendazole with food. The most serious documented risk is hepatotoxicity (liver injury), which is rare but has been reported in case studies. Monitoring liver function tests (ALT, AST, bilirubin) is recommended, especially for long-term use. Neutropenia (low white blood cell count) has been reported rarely.
❓ 7. Does fenbendazole work for small cell lung cancer (SCLC)?
Answer: Direct preclinical research on fenbendazole in SCLC models is notably limited. No published studies have tested fenbendazole in SCLC cell lines or xenograft models. Joe Tippens had SCLC and reported remission, but his case is anecdotal and he was receiving conventional treatment concurrently. SCLC typically has mutated/deleted p53 (TP53 + RB1 co-mutation), which may limit the effectiveness of fenbendazole's p53-stabilization mechanism. The microtubule disruption and glucose metabolism mechanisms are p53-independent and may still be relevant, but this has not been experimentally validated in SCLC.
❓ 8. What is the FBZ + DADA combination, and is it better than fenbendazole alone?
Answer: Recent 2025 research explored combining fenbendazole with diisopropylamine dichloroacetate (DADA) in A549 NSCLC xenograft mice. The combination produced 50% complete tumor regression, compared to 0% for fenbendazole alone and 11.1% for DADA alone. The combination was synergistic and showed improved safety (no liver toxicity). DADA has hepatoprotective properties and targets metabolic pathways complementary to fenbendazole. However, DADA is not commercially available, and this remains a preclinical proof-of-concept that has not been tested in humans.
❓ 9. Should I use Panacur C or pharmaceutical-grade fenbendazole capsules?
Answer: Panacur C granules are widely available and low cost (Joe Tippens used this), but they are a veterinary formulation containing additives/flavorings and require measuring (1g ≈ 222mg FBZ). Pharmaceutical-grade capsules provide precise dosing (222mg, 444mg), third-party lab testing, and no veterinary additives, but are more expensive. For accuracy and quality assurance, pharmaceutical-grade capsules with certificates of analysis (CoA) are preferred. See: Where to Buy Fenbendazole.
❓ 10. Can I use fenbendazole instead of chemotherapy for lung cancer?
Answer: No. Fenbendazole should not be used as a substitute for conventional lung cancer treatment (surgery, chemotherapy, radiation, targeted therapy, immunotherapy) without professional medical guidance. There are no clinical trials proving fenbendazole is effective as a standalone cancer treatment in humans. Delaying or forgoing proven treatments can result in disease progression and worse outcomes. If you are considering integrating fenbendazole into your treatment plan, discuss it with your oncologist.
❓ 11. Is there any clinical trial data on fenbendazole for lung cancer?
Answer: As of July 2026, there are no completed, peer-reviewed clinical trials evaluating fenbendazole as a lung cancer treatment in humans. The evidence base consists of preclinical studies (cell lines and animal models) and anecdotal reports. Related research is progressing: a Phase I/II trial (NCT05318469) is evaluating ivermectin (a related antiparasitic) combined with immunotherapy in metastatic breast cancer. If successful, this could pave the way for formal fenbendazole trials in lung cancer.
❓ 12. Does fenbendazole cross the blood-brain barrier for lung cancer brain metastases?
Answer: It is unclear whether fenbendazole effectively crosses the blood-brain barrier (BBB) in humans. Some expert analyses suggest fenbendazole's limited efficacy in animal brain tumor models may be due to poor BBB penetration. Mebendazole (a closely related benzimidazole) has better-documented BBB penetration and may be a more appropriate choice for brain metastases. For patients with lung cancer brain metastases considering benzimidazole therapy, discuss mebendazole with your neuro-oncologist. See: Fenbendazole vs. Mebendazole.
❓ 13. How do I monitor safety if I'm using fenbendazole for lung cancer?
Answer: Recommended safety monitoring includes: Baseline liver function tests (LFTs) — ALT, AST, alkaline phosphatase, bilirubin — before starting fenbendazole; Periodic monitoring: Every 4-6 weeks during use; Complete blood count (CBC) at baseline and periodically to monitor for neutropenia; Stop fenbendazole immediately if ALT/AST >3× upper limit of normal (ULN); Consult physician if liver enzyme elevation or unusual symptoms occur. Always use fenbendazole under medical supervision, especially if combining with chemotherapy.
❓ 14. Can fenbendazole help with drug-resistant lung cancer?
Answer: Fenbendazole is neither a substrate nor an inhibitor of P-glycoprotein (P-gp) — a drug efflux pump that cancer cells often overexpress to create multidrug resistance (MDR). Because fenbendazole does not rely on P-gp, it may retain activity in cancer cells that have developed resistance to other microtubule-targeting drugs like paclitaxel or vinblastine. However, this is a theoretical advantage based on preclinical data; it has not been validated in drug-resistant lung cancer patients. Fenbendazole should not be used as a treatment for drug-resistant disease without clinical trial validation.
❓ 15. Where can I find more information about fenbendazole for lung cancer?
Answer: For comprehensive information, see the following evidence-based resources on Sanare Lab Science:
- Joe Tippens Protocol — detailed protocol guide
- Fenbendazole Dosage Guide — safety-focused dosing information
- Fenbendazole and Chemotherapy — drug interaction analysis
- Fenbendazole vs. Mebendazole — benzimidazole comparison
📌 Clinical Evidence and Limitations
It is critical to state clearly: there are no completed, peer-reviewed clinical trials that have validated fenbendazole as a lung cancer treatment in humans (see Fenbendazole Clinical Trials Update 2026 for the latest status). The evidence base consists of:
- Preclinical studies: Laboratory research using NSCLC cell lines (A549) and animal models has demonstrated fenbendazole's anticancer activity through microtubule disruption, glucose uptake inhibition, and p53 stabilization. These studies document mechanisms and dose-response relationships. However, laboratory efficacy does not always translate to human clinical benefit.
- Anecdotal reports: Joe Tippens' SCLC remission is the foundational anecdotal report. A 2025 case series documented three stage IV cancer patients (including one melanoma patient with lung metastases) who achieved remission using fenbendazole, but this paper was subsequently retracted due to undisclosed financial conflicts of interest. Numerous other testimonials exist across online forums (see our collection of Fenbendazole Success Stories), but these lack independent verification and control groups.
- Mechanistic plausibility: Fenbendazole's known biological activity (tubulin binding, GLUT inhibition, p53 stabilization) provides a scientifically sound rationale for anticancer effects. The mechanisms are well-characterized and align with established cancer biology. However, mechanistic plausibility alone is not proof of clinical efficacy.
The Evidence Gap: The gap between preclinical promise and clinical proof is the central challenge. Designing and funding clinical trials for repurposed veterinary drugs is difficult because fenbendazole is off-patent (no commercial incentive), regulatory pathways are unclear, and academic funding is limited.
Key Takeaways
- ✅ Preclinical NSCLC data is robust: The 2018 MD Anderson study provides solid proof-of-concept that fenbendazole has anticancer activity in NSCLC cell lines through multiple independent mechanisms (microtubules, glucose metabolism, p53).
- ⚠️ SCLC data is limited: Despite Joe Tippens' SCLC diagnosis driving public interest, direct preclinical research on fenbendazole in SCLC models is notably absent. SCLC's p53-mutant status may limit fenbendazole's p53-dependent mechanisms.
- ⭐ FBZ + DADA combination shows promise: 2025 research documented 50% complete tumor regression in A549 xenograft mice with the FBZ + DADA combination, with improved safety profile (no hepatotoxicity). This is a preclinical proof-of-concept worth watching.
- 💊 Dosing is empirical: All human dosing is based on the Joe Tippens protocol (222 mg) or user-modified schedules. Optimal human dosing for anticancer activity is unknown.
- 🩺 Chemotherapy interaction data is reassuring: Preclinical data (FBZ + docetaxel) show additive effects with no antagonism and no additional toxicity. However, CYP1A2 induction raises concerns for EGFR inhibitor interactions (erlotinib, gefitinib). Oncologist disclosure is non-negotiable.
- ⚠️ Hepatotoxicity is the primary safety concern: Drug-induced liver injury has been documented. Monitor liver function tests (ALT, AST, bilirubin) at baseline and every 4-6 weeks during use.
- 🔬 No human clinical trials exist: All lung cancer evidence remains preclinical or anecdotal. Clinical validation is urgently needed.
- ❌ Not a replacement for standard treatment: Fenbendazole should not be used as a substitute for surgery, chemotherapy, targeted therapy, or immunotherapy without clinical trial validation. Delaying proven treatments can worsen outcomes.
Disclaimer: This article is for educational purposes only. It does not constitute medical advice. All medications, supplements, and investigational therapies should only be considered under the direct supervision of a qualified oncologist or integrative medicine physician.
Shop Sanare Lab
Below are commonly referenced items. Links are provided for convenience — always review the label and consult a professional before use.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
6 / 12 / 18 mg — 100 tablets
120 capsules — with Black Pepper for absorption
Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.
🤖 AI-Assisted Content Notice
This article was researched and drafted with AI assistance. All cited studies are real, peer-reviewed publications verifiable on PubMed. Content has been reviewed for scientific accuracy. This article is for informational purposes only and does not constitute medical advice.
📋 Declaration of AI-Assisted Technology in the Writing Process
During the preparation of this article, the author(s) used Claude 3.5 Sonnet by Anthropic for the purposes of literature search assistance, initial draft organization, grammar and style refinement.
The author(s) have reviewed and edited all AI-assisted output and take full responsibility for the accuracy, integrity, and originality of the content of this publication. All medical claims have been independently verified against peer-reviewed sources by the designated medical reviewer.
In accordance with ICMJE and COPE guidelines, AI tools are not listed as authors as they cannot take accountability for the work. This disclosure follows FTC transparency requirements for digital content.
⚕️ Medical Disclaimer: This article is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay seeking it because of something you have read on this website.
References
- Dogra N, Kumar A, Mukhopadhyay T. Fenbendazole acts as a moderate microtubule destabilizing agent and causes cancer cell death by modulating multiple cellular pathways. Sci Rep, 2018. PMID: 29867127. PubMed
- Song B, Park EY, Kim KJ, Ki SH. Repurposing of benzimidazole anthelmintic drugs as cancer therapeutics. Cancers, 2022. PMID: 35884373. PubMed
- Florio R, Mortimer L, Salomone F et al.. Repurposing veterinary drugs for human cancers: a systematic review of preclinical studies. Drug Discov Today, 2023. PMID: 36878395. PubMed
- Bai RY, Staedtke V, Aprhys CM et al.. Antiparasitic mebendazole shows survival benefit in 2 preclinical models of glioblastoma multiforme. Neuro Oncol, 2011. PMID: 21727211. PubMed
- Duan Q, Liu Y, Bhattacharya S. Fenbendazole as a potential anticancer drug. Anticancer Res, 2013. PMID: 23482766. PubMed
- Mrkvová Z, Uldrijan S, Pombinho A et al.. Benzimidazoles downregulate Mdm2 and MdmX and activate p53 in MdmX overexpressing tumor cells. Molecules, 2019. PMID: 31671553. PubMed
- Park D, Lee JH, Yoon SP. Anti-cancer effects of fenbendazole on 5-fluorouracil-resistant colorectal cancer cells. Korean J Parasitol, 2022. PMID: 36041488. PubMed
- Cáñez-González KE, García-Saucedo BN, Enciso-Benavides J et al.. Evaluation of fenbendazole as an anticancer agent in tumor-bearing mice. J Cancer Res Ther, 2023. PMID: 38047367. PubMed
- Chu SW, Badar S, Morris DL, Pourgholami MH. Potent inhibition of tubulin polymerisation and proliferation of paclitaxel-resistant 1A9PTX22 human ovarian cancer cells by albendazole. Anticancer Res, 2009. PMID: 19528482. PubMed
- Nygren P, Larsson R. Drug repositioning from bench to bedside: tumour remission by the antihelmintic drug mebendazole in refractory metastatic colon cancer. Acta Oncol, 2014. PMID: 24160353. PubMed
- Huang L, Zhao L, Zhang J et al.. Antiparasitic mebendazole (MBZ) effectively overcomes cisplatin resistance in human ovarian cancer cells by inhibiting multiple cancer-associated signaling pathways. Aging, 2021. PMID: 33495418. PubMed
- Guerini AE, Triggiani L, Maddalo M et al.. Mebendazole as a candidate for drug repurposing in oncology: an extensive review of current literature. Cancers, 2019. PMID: 31540055. PubMed
- Son DS, Lee ES, Bhatt SE. Fenbendazole induces apoptosis of HL-60 cells by disrupting the integrity of the tubulin-microtubule system. Korean J Parasitol, 2020. PMID: 33227869. PubMed
Related Resources
Evidence-based guides for understanding fenbendazole protocols, safety, and comparisons.
Complete guide to the original protocol — dosages, supplements, safety, and evidence
Can they be combined safely? Drug interaction analysis and practical guidance
Safety-focused dosing information, monitoring, and quality verification
Disclaimer: Educational resources only. Always consult a licensed oncologist for medical guidance.
Shop Sanare Lab
Below are commonly referenced items. Links are provided for convenience — always review the label and consult a professional before use.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
6 / 12 / 18 mg — 100 tablets
120 capsules — with Black Pepper for absorption
Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.
Shop Sanare Lab
Below are commonly referenced items. Links are provided for convenience — always review the label and consult a professional before use.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
6 / 12 / 18 mg — 100 tablets
120 capsules — with Black Pepper for absorption
Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.