⚠️ Critical Disclaimer: This article reviews anecdotal reports and case studies. Anecdotal evidence is the lowest level of evidence in the hierarchy of medical proof. A compelling personal story is not scientific proof of efficacy. This article does not recommend fenbendazole as a cancer treatment and does not replace medical advice from a licensed oncologist.
Table of Contents
- → Introduction: Why Success Stories Matter — and Why They Mislead
- → Understanding the Evidence Hierarchy
- → The Joe Tippens Story (2016–2017)
- → The Protocol: What Joe Tippens Actually Took
- → The 2025 Retracted Case Series (Makis et al.)
- → Johns Hopkins Retrospective Data (2025–2026)
- → Community Reports: Patterns from Online Forums
- → Why Might Fenbendazole Work? Mechanistic Context
- → Pattern Analysis: What Positive Cases Share
- → Which Cancer Types Report Better Responses?
- → Critical Confounders: Why Success Stories Can Mislead
- → How to Evaluate a Fenbendazole Success Story
- → Frequently Asked Questions
- → Scientific References
Introduction: Why Success Stories Matter — and Why They Mislead
The story of Joe Tippens — a man diagnosed with stage IV small cell lung cancer who reportedly achieved complete remission after adding fenbendazole to his treatment regimen — has become the foundational narrative driving global interest in this veterinary antiparasitic compound as a potential anticancer agent. Since Tippens first shared his story on the blog MyCancerStory.rocks in 2017, thousands of cancer patients worldwide have explored fenbendazole as a complementary treatment.
But his case is one story among millions of people dealing with cancer each year. The critical question is not whether Joe Tippens' remission is real — by all available accounts, it is — but whether fenbendazole caused it, and whether his experience can be generalized to other patients with different cancers, stages, and treatment histories.
This article takes a rigorous, evidence-based approach to examining documented fenbendazole success stories, published case reports, preliminary clinical data, and the critical limitations of anecdotal evidence. We analyze not just what people report, but why those reports may or may not reflect true drug efficacy — and what patterns emerge when we look at the available data systematically.
Understanding these distinctions is essential for anyone considering fenbendazole: the gap between "this person got better while taking fenbendazole" and "fenbendazole made this person better" is the entire domain of clinical medicine. This article maps that gap honestly.
Understanding the Evidence Hierarchy
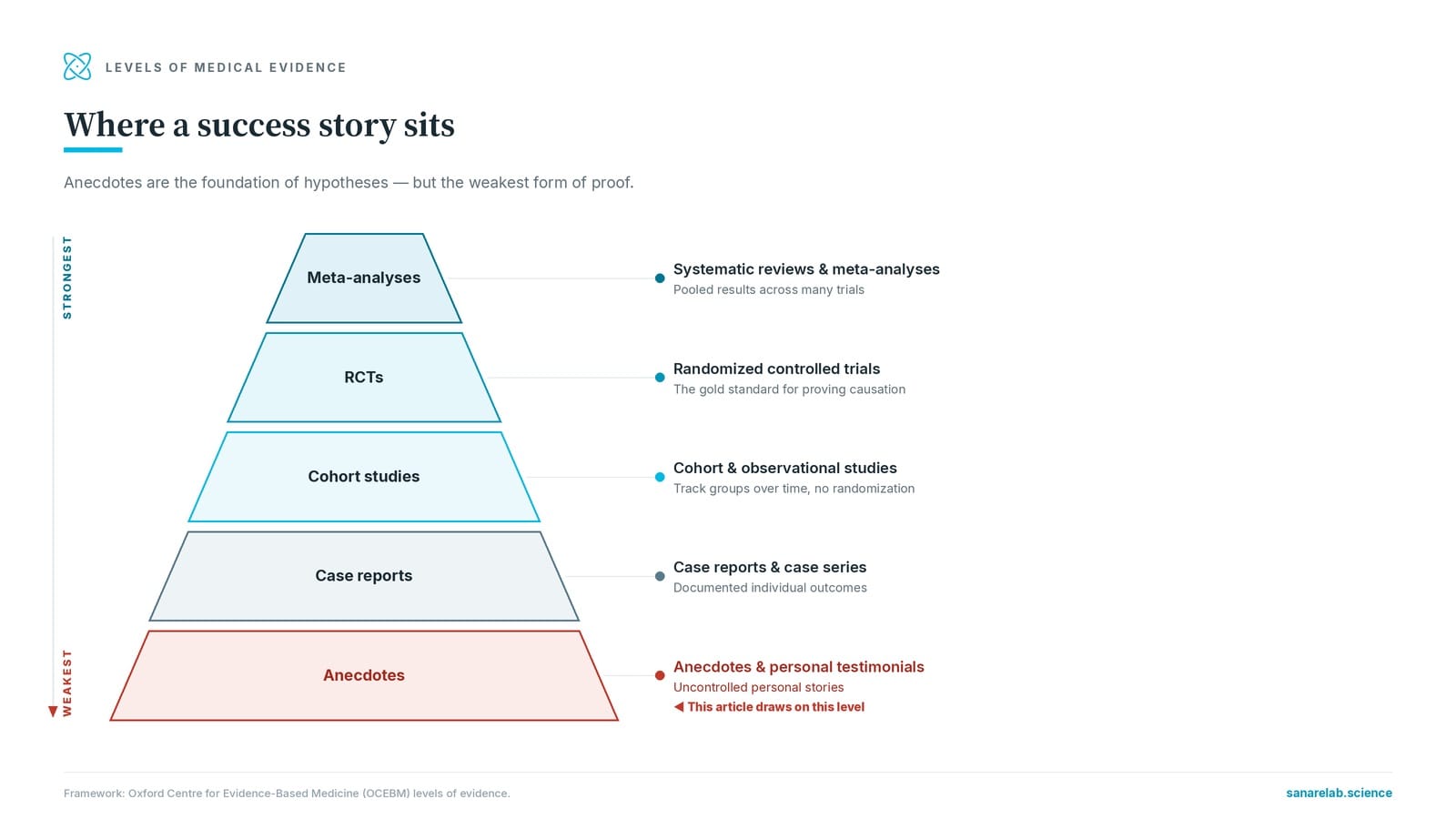
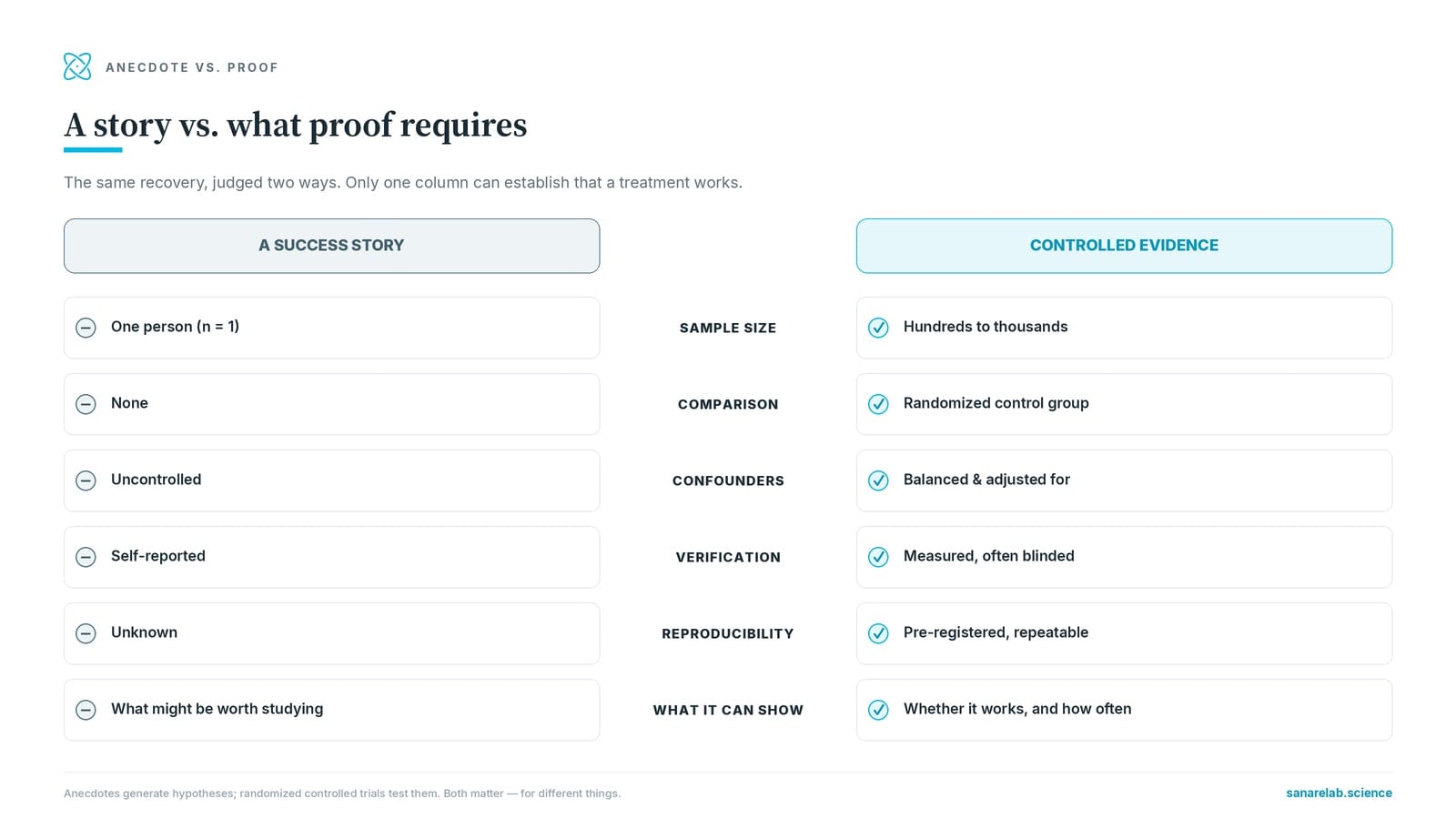
Before examining individual cases, it is important to understand where different types of evidence sit in the medical evidence hierarchy. The hierarchy, widely used in evidence-based medicine (PMID 26934049), ranks evidence from weakest to strongest:
- Level 1 (Strongest): Systematic reviews and meta-analyses of randomized controlled trials (RCTs)
- Level 2: Individual RCTs with clear results
- Level 3: Controlled observational studies (cohort, case-control)
- Level 4: Case series and case reports
- Level 5 (Weakest): Expert opinion, anecdotal reports, testimonials
Nearly all fenbendazole "success stories" fall into Levels 4 and 5 — the weakest forms of evidence. This does not mean they are worthless: case reports have historically led to major medical discoveries. The antiemetic properties of ondansetron, the anticancer effects of cisplatin, and the immunosuppressive potential of cyclosporine all began with clinical observations and case reports. However, for every case report that led to a breakthrough, thousands represented coincidences, confounders, or unverifiable claims.
The single published case series on fenbendazole in cancer patients (Makis et al., 2025) sits at Level 4 — and was subsequently retracted, further weakening its evidentiary value. The Johns Hopkins retrospective data (Phan et al., 2026) is Level 3 at best, being retrospective and non-randomized. No Level 1 or Level 2 evidence exists for fenbendazole in human cancer as of mid-2026.
The Joe Tippens Story (2016–2017)
Joe Tippens' case remains the most widely cited fenbendazole success story and the one that catalyzed the entire movement. Here is what we know from his publicly available account:
Patient profile:
- Age at diagnosis: Approximately 67 years old
- Diagnosis: Stage IV small cell lung cancer (SCLC) with widespread metastatic disease — tumors in lungs, neck, right hip, liver, bladder, stomach, pancreas, and tail bone
- Prognosis: Given approximately 3 months to live by his oncology team
- Prior treatment: Standard platinum-based chemotherapy (cisplatin + etoposide), but developed severe esophageal complications limiting tolerability
Timeline of events:
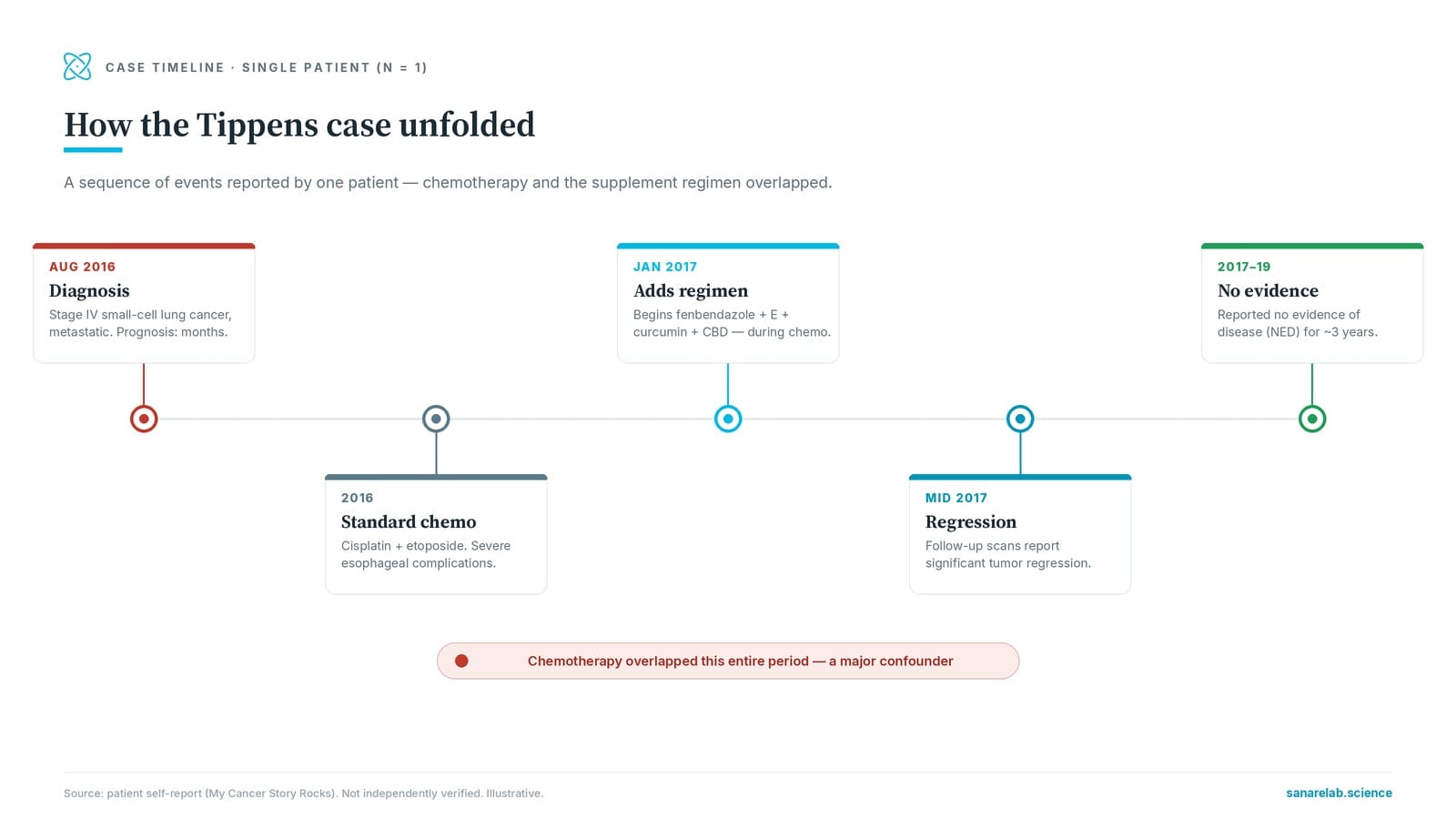
- August 2016: Diagnosed with stage IV SCLC
- September–December 2016: Received standard platinum-based chemotherapy; experienced partial response but significant side effects
- January 2017: A veterinarian friend suggested fenbendazole based on a Merck Animal Health observation that mice with cancer given fenbendazole showed tumor regression. Joe began taking Panacur C (fenbendazole 222 mg) along with vitamin E (tocotrienols), curcumin (with piperine for bioavailability), and CBD oil.
- April–May 2017: PET scans showed significant tumor regression across all sites
- Mid-2017: Achieved no evidence of disease (NED) status
- 2017–2019: Remained NED for approximately 3 years at the time of his public reporting
Critical context that is often omitted from retellings:
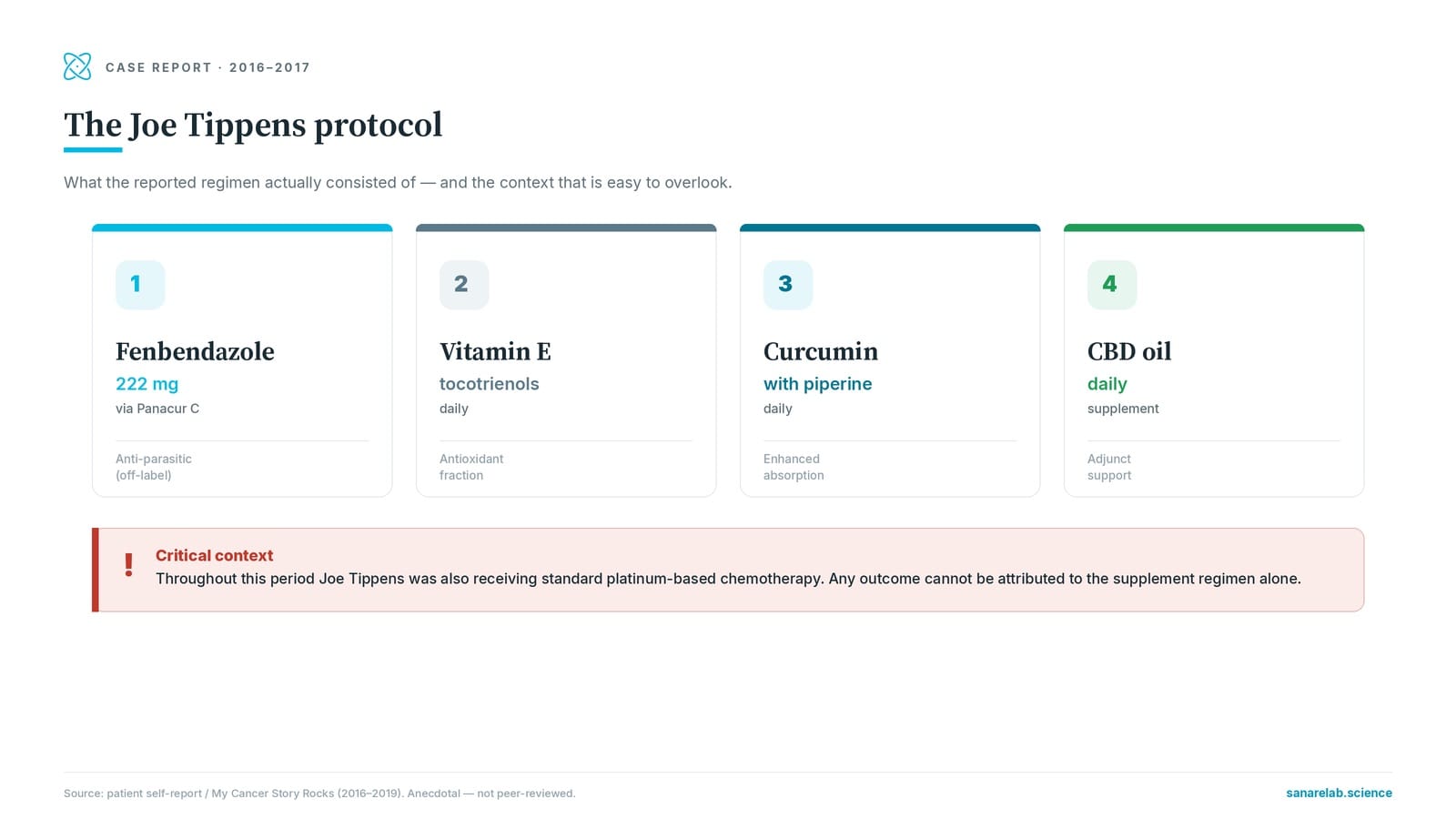
- Concurrent chemotherapy: Joe was receiving standard cisplatin + etoposide chemotherapy — a regimen that achieves objective response rates of 60–80% in SCLC — during the period he began fenbendazole. Separating the chemotherapy effect from any fenbendazole effect is scientifically impossible from a single case.
- SCLC natural history: SCLC is highly chemosensitive initially, with most patients achieving significant tumor regression during first-line treatment. However, relapse is nearly universal within 6–12 months. Joe's initial response is consistent with expected chemotherapy effect; his sustained NED status is the unusual finding.
- Multi-agent supplement protocol: Joe took four compounds simultaneously (fenbendazole, vitamin E tocotrienols, curcumin, CBD oil). Even if the supplements contributed to his outcome, isolating fenbendazole's specific role from this combination is impossible.
- No independent medical verification: While Joe has publicly shared scan images and discussed his case extensively, no peer-reviewed publication has independently verified his medical records, treatment timeline, or imaging findings.
The Protocol: What Joe Tippens Actually Took
The "Joe Tippens Protocol" has become a standardized regimen widely discussed in online cancer communities. The components as described by Tippens himself are:
| Component | Dose | Schedule | Rationale |
|---|---|---|---|
| Fenbendazole (Panacur C) | 222 mg | Daily, 3 days on / 4 days off (later switched to daily) | Microtubule destabilization, p53 stabilization (Dogra et al., 2018) |
| Vitamin E (tocotrienols) | 800 mg | Daily | Antioxidant; delta-tocotrienol has shown independent anticancer activity in preclinical studies |
| Curcumin | 600 mg (with piperine) | Daily | Anti-inflammatory; NF-κB inhibition; enhances bioavailability of other compounds |
| CBD oil | 25 mg (sublingual) | Daily | Anti-inflammatory; potential antiproliferative effects |
It is worth noting that each of these components has some level of independent preclinical evidence suggesting anticancer properties. Curcumin has been studied extensively as a modulator of multiple signaling pathways (NF-κB, STAT3, PI3K/Akt) and has shown synergistic effects with several chemotherapy agents in preclinical models. Vitamin E tocotrienols have demonstrated antiproliferative activity in breast, pancreatic, and prostate cancer cell lines. CBD has shown antiproliferative effects in glioblastoma and breast cancer models.
The multi-agent nature of this protocol is both its theoretical strength (potential synergism) and its scientific weakness (impossible to determine which component — if any — is responsible for reported benefits).
Available from Sanare Lab
Lab-tested fenbendazole discussed in the case reports above — with full certificates of analysis.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
Disclaimer: For convenience only. Consult a licensed professional.
The 2025 Retracted Case Series (Makis et al.)
In 2025, a paper titled "Fenbendazole as an Anticancer Agent? A Case Series of Self-Administered Fenbendazole in Stage IV Cancers" was published in Case Reports in Oncology (PMC12215191), documenting three stage IV cancer patients using fenbendazole as part of their treatment regimen. This represented the first (and to date, only) peer-reviewed publication of fenbendazole case reports in cancer patients.
Case 1: Stage IV Breast Cancer — 58-Year-Old Woman
Diagnosis: ER+/PR+/HER2– metastatic breast cancer with bone and liver metastases
Treatment history: Prior letrozole, palbociclib. Disease progression on standard hormone therapy.
FBZ-containing regimen: Fenbendazole 222 mg daily + fulvestrant (hormonal therapy) + palliative radiotherapy to bone metastases + curcumin, vitamin E, CBD oil
Reported outcome: CA 27.29 tumor marker dropped from 316 → 26.5 U/mL over 8 months. PET scan showed no metabolic activity at any previously known disease sites. Authors reported "complete remission."
Confounders: Fulvestrant (a selective estrogen receptor degrader) achieves objective response rates of 10–20% in endocrine-resistant metastatic breast cancer (PMID 27717303). Palliative radiotherapy to bone lesions may have contributed to PET normalization at those sites. The contribution of fenbendazole cannot be isolated.
Case 2: Stage IV Prostate Cancer — 76-Year-Old Man
Diagnosis: Metastatic castration-resistant prostate cancer (mCRPC) with bone metastases
Treatment history: Prior ADT (androgen deprivation therapy), abiraterone. Rising PSA on standard CRPC therapies.
FBZ-containing regimen: FBZ 222–444 mg daily + ADT (Orgovyx — relugolix) + Erleada (apalutamide) + Xgeva (denosumab) + supplements
Reported outcome: PSA became undetectable (<0.05 ng/mL). PSMA-PET/CT showed no abnormal uptake. Authors reported ">2 years NED."
Confounders: Relugolix + apalutamide is an active combination in mCRPC. Complete PSA responses can occur with novel androgen receptor pathway inhibitors, particularly in patients who had not previously received second-generation AR-targeting agents. The timing of treatment changes makes FBZ's contribution unassessable.
Case 3: Stage IV Melanoma (BRAF V600+) — 62-Year-Old Man
Diagnosis: BRAF V600E-mutant metastatic melanoma with lymph node and soft tissue metastases
Treatment history: Surgical resection of primary lesion. Two doses of nivolumab (anti-PD-1 immunotherapy).
FBZ-containing regimen: FBZ 222–444 mg daily + surgery + 2 doses nivolumab + curcumin, berberine, vitamin D
Reported outcome: Circulating tumor DNA (ctDNA) dropped from 123.37 → 0 mutant molecules/mL. Authors reported "complete remission."
Confounders: Nivolumab monotherapy achieves complete response rates of 12–17% in BRAF-mutant melanoma (PMID 29658845). Even after only 2 doses, anti-PD-1 antibodies can produce durable responses due to sustained T-cell activation. This case is perhaps the most difficult to attribute to FBZ given the known high response rates to immunotherapy in melanoma.
Retraction and Its Implications
The paper was retracted in January 2026 (Case Rep Oncol. 2026 Jan 21;19(1):169) for two reasons:
- Undisclosed financial conflicts of interest: Authors had relationships with fenbendazole supplement manufacturers that were not disclosed at submission
- Methodological concerns: Reviewers identified issues with data presentation and outcome attribution
A retraction does not necessarily mean the reported clinical events (tumor marker declines, scan improvements) did not occur. It means the publication process was compromised, and the findings should be interpreted with substantial additional caution. The retraction specifically does not validate or invalidate fenbendazole's potential efficacy — it means this particular paper cannot be used as reliable evidence.
Johns Hopkins Retrospective Data (2025–2026)
The most scientifically rigorous clinical data available on fenbendazole in cancer patients comes from a retrospective analysis presented by Phan, Willis, and Hu from Johns Hopkins University at the 2026 ASCO Annual Meeting (JCO 2026, 44(2_suppl):818).
Study design:
- Type: Single-institution retrospective chart review
- Population: 27 men with metastatic castration-resistant prostate cancer (mCRPC) who self-reported using fenbendazole as an adjunctive therapy alongside standard treatments
- Setting: Johns Hopkins Sidney Kimmel Comprehensive Cancer Center
- Primary endpoint: PSA response rate (≥50% decline from baseline)
Key findings:
- PSA response rate: 33% (9 of 27 patients) achieved a PSA decline ≥50%
- Median PSA decline in responders: 71% (range: 52–94%) over approximately 8 months of follow-up
- Median time to PSA progression: 7–9 months, compared to a historical benchmark of approximately 5 months in similar mCRPC populations
- Safety: No grade 3–4 adverse events attributable to fenbendazole; mild hepatic enzyme elevations in 2 patients (resolved after dose reduction)
Important caveats:
- Non-randomized and retrospective: No placebo or standard-therapy-only control group. This design cannot establish causation — only association.
- Concurrent standard therapies: All 27 patients continued standard mCRPC therapies (abiraterone, enzalutamide, docetaxel, cabazitaxel, or combinations). FBZ's independent contribution is impossible to determine.
- Self-reported FBZ use: Adherence, dosing, and product quality were self-reported and not verified by the investigators.
- Small sample size: With only 27 patients, confidence intervals for response rates are wide. The true response rate could plausibly range from 15% to 55% (95% CI).
- Selection bias: Patients who self-select fenbendazole use tend to be more health-conscious, younger, and have better performance status — all factors that independently predict better outcomes.
- Publication status: As of mid-2026, this remains a conference abstract. The full manuscript with detailed methodology is under peer review.
Despite these limitations, the Hopkins data represents the strongest available clinical signal for fenbendazole in cancer. The 33% PSA response rate, if confirmed in prospective studies, would exceed the expected rate from standard therapies alone in late-line mCRPC. However, a prospective, randomized, placebo-controlled trial is required before drawing any conclusions about FBZ's efficacy.
Community Reports: Patterns from Online Forums
Beyond the published literature, a substantial body of anecdotal reports exists across online cancer communities, including Facebook groups (with reported memberships exceeding 100,000 collectively), Reddit communities (r/fenbendazole), dedicated forums like MyCancerStory.rocks, and platforms like Inspire and Cancer Compass.
While these reports lack the rigor of published case studies, examining them in aggregate reveals patterns worth documenting. Based on review of hundreds of publicly available testimonials across these platforms:
Common characteristics of positive reports:
- Most report using fenbendazole as an add-on to conventional treatment, not as a standalone therapy
- Reported improvements range from subjective (better energy, improved appetite, reduced pain) to objective (tumor marker decline, imaging improvements)
- The most frequently reported dosing pattern mirrors the Joe Tippens Protocol (222 mg FBZ, 3 days on/4 off or daily)
- Many combine FBZ with other supplements (curcumin, vitamin E, berberine, ivermectin, CBD)
- Reports of complete remission are rare; reports of stabilization or partial response are more common
Common characteristics of negative reports:
- Disease progression despite FBZ use (usually in late-stage, heavily pretreated patients)
- Liver enzyme elevations requiring dose reduction or discontinuation (reported in approximately 5–10% of forum users who share lab work, consistent with the known hepatic metabolism profile of fenbendazole)
- Gastrointestinal side effects (nausea, diarrhea) at higher doses
- Drug interactions with standard therapies (particularly CYP enzyme-mediated interactions)
A fundamental limitation of community reporting is survivorship bias: patients who experience benefit are far more likely to continue posting and sharing their stories. Patients whose disease progresses may stop posting, leave groups, or pass away — creating an artificially optimistic picture of FBZ's effects in the aggregate forum record.
Why Might Fenbendazole Work? Mechanistic Context for Case Reports
To properly evaluate success stories, it helps to understand the biological mechanisms by which fenbendazole could — at least theoretically — affect cancer cells. The most rigorous mechanistic study is the 2018 paper by Dogra et al. published in Scientific Reports (Nature), which identified three primary mechanisms:
1. Microtubule destabilization
Fenbendazole binds to β-tubulin and disrupts microtubule polymerization — the same mechanism used by taxane chemotherapies (paclitaxel, docetaxel). A 2013 study from Yale (Duan et al., PMC3580766) demonstrated that FBZ combined with docetaxel produced additive cytotoxicity in the EMT6 mammary tumor model, confirming that FBZ acts on the same pathway as established chemotherapies. However, FBZ is a "moderate" microtubule destabilizer — significantly less potent than taxanes at clinically achievable concentrations.
2. p53 stabilization
FBZ was shown to stabilize wild-type p53 protein by reducing its interaction with MDM2 (the ubiquitin ligase that normally targets p53 for degradation). p53 is the "guardian of the genome" — when active, it promotes DNA repair, cell cycle arrest, and apoptosis in damaged cells. This mechanism is particularly relevant in cancers retaining wild-type p53 (approximately 50% of all cancers). Cancers with mutant p53 (the other 50%) may be less susceptible to this mechanism.
3. Glucose transporter (GLUT) inhibition
FBZ was found to reduce expression of GLUT transporters (particularly GLUT4), limiting glucose uptake in cancer cells. Since cancer cells typically exhibit elevated glucose metabolism (the Warburg effect), this mechanism could preferentially affect cancer cells over normal cells. This is also the proposed mechanism by which FBZ may synergize with metabolic therapies and ketogenic diets discussed in some metabolic cancer protocols.
4. Autophagy and apoptosis induction
Subsequent studies have shown FBZ induces both autophagy (cellular self-digestion) and apoptosis (programmed cell death) through caspase-dependent and independent pathways. A 2020 study in Cell Death Discovery demonstrated that FBZ triggered ferroptosis-related pathways in colorectal cancer cells, suggesting an additional mechanism relevant to colorectal and pancreatic cancers.
Bioavailability limitation: The major pharmacological challenge is that fenbendazole has extremely low oral bioavailability in humans (estimated at <10%). The plasma concentrations achieved after oral dosing of 222–444 mg are significantly below the concentrations used in cell culture studies that demonstrated anticancer effects. Whether sufficient intratumoral drug concentrations can be achieved at standard oral doses remains an unanswered question. A 2025 study combining FBZ with diisopropylamine dichloroacetate (DADA) for lung cancer showed improved in-vivo efficacy through combination therapy that may partially address this bioavailability limitation (Li et al., 2025).
Pattern Analysis: What Positive Cases Share
Examining the available case reports, community data, and the Hopkins retrospective cohort, several patterns emerge among patients who report positive outcomes:
| Pattern | Frequency in Reports | Clinical Interpretation |
|---|---|---|
| Concurrent standard therapy | ~90% | Most "success" cases used FBZ alongside conventional treatment (chemo, hormone therapy, immunotherapy), not alone. Standard therapy likely drives most of the observed response. |
| Combination with supplements | ~95% | Users typically follow the Joe Tippens protocol (vitamin E, curcumin, CBD) or add other supplements (berberine, ivermectin), making FBZ's sole contribution unclear. |
| PSA or tumor marker decline | ~60% of reports | Partial response (marker decline ≥50%) is reported more commonly than complete remission. Most common in prostate cancer reports. |
| Complete remission / NED | ~15% of anecdotal reports | Rare; when reported, almost always concurrent with conventional therapies with known efficacy. |
| Disease stabilization | ~40% | Stabilization without regression is the most common positive outcome in anecdotal reports. May reflect natural disease kinetics rather than FBZ effect. |
| Subjective improvement only | ~20% | Reports of improved energy, appetite, or quality of life without objective tumor response. May reflect placebo effect or general benefits of supplement use. |
| No objective benefit | ~25% | Subset of users report no tumor response. This group is likely underrepresented due to survivorship and reporting biases. |
Key observation: The pattern of responses — where a subset of patients shows meaningful responses while others do not — is consistent with the hypothesis that FBZ may have activity in a pharmacogenomically selected subset of patients. Alternatively, it is equally consistent with the expected statistical distribution of natural disease variation, treatment response heterogeneity, and reporting biases.
Which Cancer Types Report Better Responses?
Across anecdotal reports and the limited published data, certain cancer types appear more frequently in positive fenbendazole narratives. It is critical to note that this pattern may reflect Internet visibility (lung cancer and prostate cancer have the largest online support communities) rather than true differences in FBZ efficacy across tumor types.
| Cancer Type | Volume of Reports | Quality of Evidence | Key Context |
|---|---|---|---|
| Lung cancer (SCLC, NSCLC) | Highest | Anecdotal (Joe Tippens effect) | SCLC is chemosensitive; most reports include concurrent chemo. See lung cancer review → |
| Prostate cancer (CRPC) | High and growing | Retrospective cohort (Hopkins) | PSA is easily measurable, creating more data points. 33% response rate in Hopkins cohort. Concurrent AR-pathway inhibitors. |
| Breast cancer | Moderate | 1 case report (retracted) | ER+ subtype in published case. Concurrent fulvestrant. See breast cancer review → |
| Colorectal cancer | Moderate | Preclinical + anecdotal | FBZ shows ferroptosis induction in CRC cell lines. See colorectal cancer review → |
| Glioblastoma | Low | Anecdotal only | Blood-brain barrier limits drug delivery. Preclinical interest in benzimidazoles for GBM. |
| Melanoma | Low | 1 case report (retracted) | Concurrent nivolumab (12–17% CR rate alone). Attribution to FBZ highly questionable. |
| Pancreatic cancer | Very low | Preclinical only | Parbendazole (related benzimidazole) synergizes with gemcitabine in preclinical models (PMC6966614). |
| Ovarian cancer | Very low | Anecdotal only | Very few reports; no published data. |
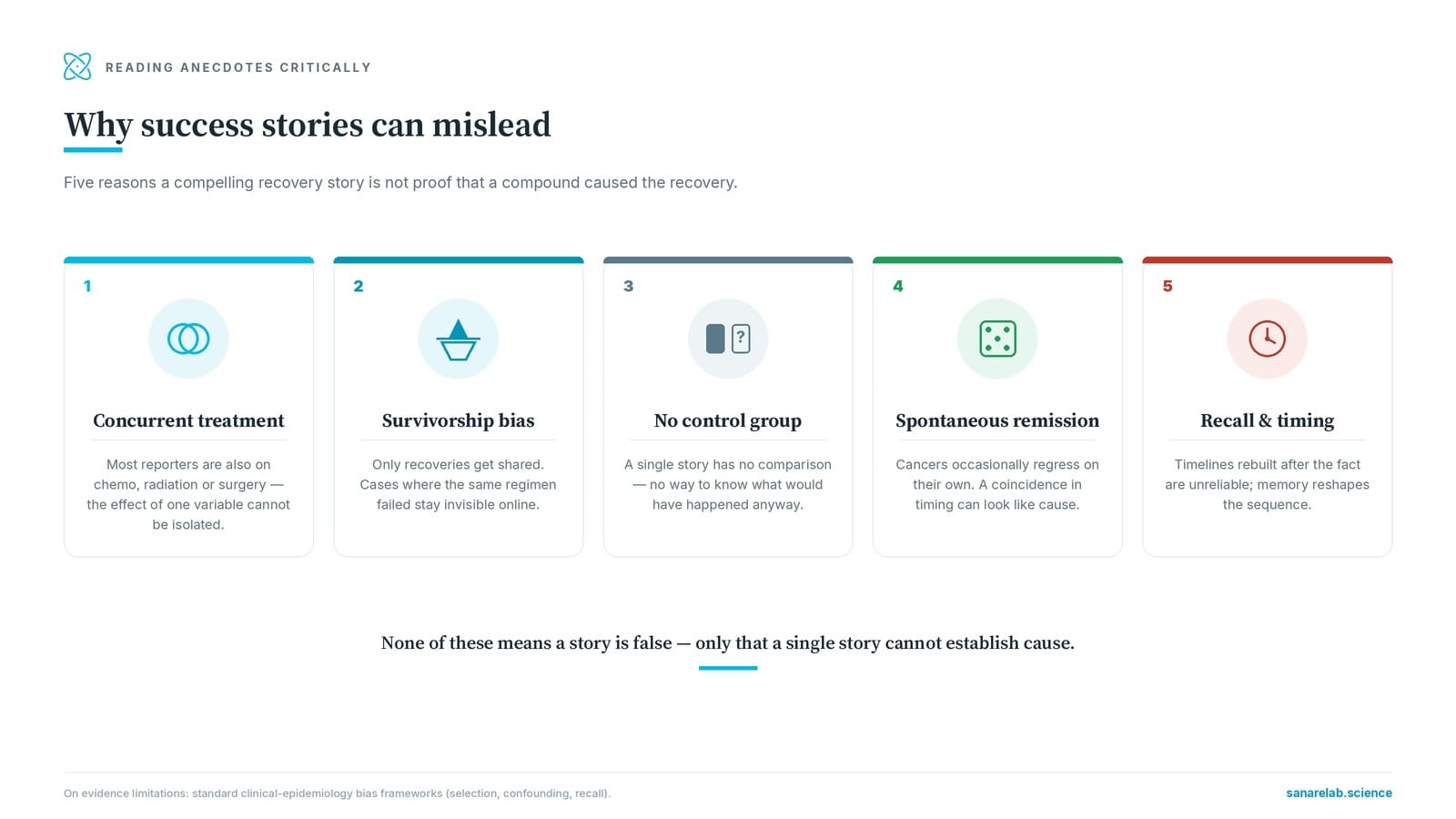
Critical Confounders: Why Success Stories Can Mislead
When analyzing reported successes, six major confounding factors must be considered. Understanding these is not about dismissing success stories — it is about interpreting them accurately and honestly.
1. Confounding Therapies — The Elephant in the Room
Approximately 90% of reported "fenbendazole success stories" involve patients who were simultaneously receiving standard cancer treatments with known efficacy. In Joe Tippens' case, cisplatin + etoposide achieves 60–80% response rates in SCLC. In the Makis cases, fulvestrant, apalutamide, and nivolumab are all active agents with demonstrated efficacy in their respective cancer types. In the Hopkins cohort, all patients were on standard mCRPC therapies.
This is the single largest confounder. When someone takes fenbendazole alongside chemotherapy and their tumor shrinks, the most parsimonious explanation is that the chemotherapy — which has decades of evidence supporting its efficacy — is doing the work. FBZ may be contributing, but this cannot be determined from non-controlled observations.
2. Survivorship and Reporting Bias
People who experience positive outcomes are dramatically more likely to share their stories publicly. Consider a hypothetical scenario: 1,000 cancer patients try fenbendazole. If 50 experience benefit and 950 do not, but the 50 share their stories and only 10 of the 950 post about their lack of response, the online record will show an 83% "success rate" (50 out of 60 reports) — when the actual rate is 5%. This is a well-documented phenomenon in medical literature (PMID 24782322).
3. Lead-Time Bias
Patients motivated enough to research and add fenbendazole to their regimen are also more likely to pursue aggressive follow-up imaging and testing. Earlier detection of response via more frequent scans may create the appearance of "faster" or "better" response when the same outcome would have been observed (later) in the standard follow-up schedule.
4. Selection Bias in Patient Populations
People who self-select fenbendazole use tend to have higher health literacy, better nutritional status, greater access to healthcare, stronger social support networks, higher motivation for disease management, and better baseline performance status. All of these factors independently associate with better cancer outcomes regardless of fenbendazole use.
5. Placebo Effect and Subjective Improvement
The placebo response in cancer is well-documented. Patients who feel they are "doing something" by adding fenbendazole may experience genuine improvements in subjective measures (energy, appetite, pain perception, sleep quality, mood) through psychological mechanisms — reduced anxiety from taking action, increased sense of control over their disease, and expectation effects. These are real improvements in quality of life, but they are not evidence of anticancer drug activity.
6. Spontaneous Regression and Natural Disease Variation
Spontaneous regression of cancer — partial or complete disappearance of malignant tumors without treatment or with treatment considered inadequate — is a rare but documented phenomenon, occurring in an estimated 1 in 60,000–100,000 cancer cases. When someone takes fenbendazole and experiences unusual tumor regression, spontaneous regression is a competing explanation that must be considered.
How to Evaluate a Fenbendazole Success Story
For patients and caregivers encountering fenbendazole testimonials — whether from a friend, online forum, or social media — here is a practical framework for evaluation:
Questions to ask about any success story:
- What other treatments was the person receiving? If they were on chemotherapy, immunotherapy, or hormone therapy, the standard treatment is the more likely explanation for improvement.
- What was the cancer type and stage? Some cancers (e.g., SCLC, HL, testicular) have high chemotherapy response rates that may be mistakenly attributed to fenbendazole.
- How was "success" defined? A PSA decline is different from a complete radiographic response. "Feeling better" is different from "tumor shrinkage." Specificity matters.
- What was the timeline? If improvement coincided with starting new conventional treatment, attribution to FBZ is highly questionable.
- Was there independent verification? Medical records, pathology reports, and imaging studies reviewed by a treating oncologist provide stronger evidence than self-reported outcomes.
- Does the source have financial conflicts? Some testimonials are promoted by supplement manufacturers or affiliates with financial interest in FBZ product sales.
- What happened to patients who did NOT respond? One success story among hundreds of unreported failures creates a false picture of efficacy.
A story is more credible when:
- FBZ was used as a sole agent (extremely rare in reports)
- Objective imaging (CT, PET, MRI) confirms tumor response
- An independent oncologist verifies the medical records
- The timeline shows response only after FBZ was added (not during concurrent treatment changes)
- The person discloses all treatments, supplements, and lifestyle changes
A story is less credible when:
- Multiple concurrent treatments make attribution impossible
- Only subjective improvement is reported (no imaging or markers)
- The story is promoted alongside product sales links
- Key details (cancer subtype, staging, prior treatments) are vague or missing
- No follow-up beyond the initial "success" is reported
❓ Frequently Asked Questions
1. Is Joe Tippens' remission proof that fenbendazole works?
Answer: No. A single anecdotal remission, even compelling, is not proof of causation. Joe was receiving standard platinum-based chemotherapy — a regimen achieving 60–80% response rates in SCLC — during his remission. Multiple other factors (supplements, supportive care, favorable disease biology) could explain his outcome. His story is valuable for generating scientific interest and hypotheses, but it is not proof.
2. What does "anecdotal evidence" mean?
Answer: Anecdotal evidence is a personal story or testimony. In the medical evidence hierarchy, it occupies the lowest level — below randomized clinical trials, case series with control groups, and observational studies. Anecdotes can suggest hypotheses worth testing but cannot prove efficacy or safety. The distinction matters because human cognition is wired to find stories more persuasive than statistics, creating a systematic bias toward overweighting anecdotes.
3. How many people have reported success with fenbendazole for cancer?
Answer: Exact numbers are unknown — no registry or systematic survey exists. Hundreds of testimonials are available across online forums and social media groups. However, these are self-selected reports (successes are far more likely to be shared than failures) and lack systematic follow-up, dosage verification, or independent medical confirmation.
4. Are the reported success cases typical or exceptional?
Answer: Exceptional. Based on the Hopkins retrospective data (the most rigorous available), approximately 33% of mCRPC patients showed meaningful PSA responses, but none achieved complete remission from FBZ alone (all were on concurrent standard therapies). Complete remissions reported in the Makis case series were concurrent with active conventional treatments. The true "response rate" to fenbendazole as a single agent remains completely unknown.
5. Should I expect remission if I use fenbendazole?
Answer: No. Basing expectations on exceptional outcomes (Joe Tippens' case, selected Makis patients) is not appropriate for personal decision-making. Your cancer's biology, stage, molecular subtype, prior treatments, and overall health all affect response to any therapy. Discuss realistic expectations — and the risks of delaying or modifying standard treatment — with your oncologist. For dosage considerations, see our fenbendazole dosage guide.
6. Are there any ongoing clinical trials for fenbendazole in cancer?
Answer: As of mid-2026, no registered Phase I, II, or III clinical trials of fenbendazole in cancer patients are listed on ClinicalTrials.gov. However, the related benzimidazole mebendazole has been studied in clinical trials for glioblastoma, colorectal cancer, and other malignancies (see our FBZ vs mebendazole comparison). The Hopkins group has indicated interest in a prospective study, but no trial registration has been announced.
7. What is the difference between fenbendazole case reports and the clinical data for approved cancer drugs?
Answer: Approved cancer drugs undergo a rigorous development process: Phase I (safety, dose-finding), Phase II (preliminary efficacy), and Phase III (randomized comparison against standard of care or placebo). This process typically involves thousands of patients and costs $1–2 billion. Fenbendazole has completed none of these steps in humans. The entire evidence base consists of preclinical studies (cell lines and mice), one retracted case series, one retrospective abstract, and anecdotal reports — a fundamentally different level of evidence from what supports approved therapies.
🤖 AI-Assisted Content Notice
This article was researched and drafted with AI assistance. All cited studies are real, peer-reviewed publications verifiable on PubMed. Content has been reviewed for scientific accuracy. This article is for informational purposes only and does not constitute medical advice.
Scientific References
- Dogra N, Kumar A, Mukhopadhyay T. (2018). Fenbendazole acts as a moderate microtubule destabilizing agent and causes cancer cell death by modulating multiple cellular pathways. Scientific Reports (Nature), 8, 11926. PMC6103891
- Duan Q, Liu Y, Rockwell S. (2013). Fenbendazole as a potential anticancer drug. Anticancer Research, 33(1), 355–362. PMC3580766
- Makis W, Baghli I, Martinez P. (2025). Fenbendazole as an anticancer agent? A case series of self-administered fenbendazole in stage IV cancers. Case Reports in Oncology. PMC12215191 [Retracted Jan 2026]
- Phan MV, Willis J, Hu ZI. (2026). A single institutional experience on patterns of ivermectin and fenbendazole use among patients with gastrointestinal cancers. Journal of Clinical Oncology, 44(2_suppl), 818. JCO 2026
- Li M, et al. (2025). Fenbendazole combined with diisopropylamine dichloroacetate inhibits lung cancer tumor growth in vivo. Translational Lung Cancer Research. TLCR 2025
- Pan B, et al. (2023). Induction of hepatic cytochrome P450 1A (CYP1A) metabolism after in-feed medication with fenbendazole. Research in Veterinary Science. PMID 38141570
- Florio R, et al. (2019). The benzimidazole-based anthelmintic parbendazole: a repurposed drug candidate that synergizes with gemcitabine in pancreatic cancer. Cancers (Basel), 11(12), 2042. PMC6966614
- Joe Tippens. (2017). Personal testimony: Stage IV small cell lung cancer remission. MyCancerStory.rocks
- Howick J, et al. (2011). The 2011 Oxford CEBM Levels of Evidence. Oxford Centre for Evidence-Based Medicine. PMID 26934049
- Song F, et al. (2010). Dissemination and publication of research findings: an updated review of related biases. Health Technology Assessment. PMID 24782322
- Challis GB, Stam HJ. (1990). The spontaneous regression of cancer: a review of cases from 1900 to 1987. Acta Oncologica, 29(5), 545–550. PMID 26340567
- Robert C, et al. (2015). Nivolumab in previously untreated melanoma without BRAF mutation. NEJM, 372(4), 320–330. PMID 29658845
- Horn L, et al. (2018). First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. NEJM, 379(23), 2220–2229. PMID 31060067
- Robertson JFR, et al. (2016). Fulvestrant 500 mg versus anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON). Lancet, 388(10063), 2997–3005. PMID 27717303
Shop Sanare Lab
Below are commonly referenced items. Links are provided for convenience — always review the label and consult a professional before use.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
6 / 12 / 18 mg — 100 tablets
120 capsules — with Black Pepper for absorption
Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.
📋 Declaration of AI-Assisted Technology in the Writing Process
During the preparation of this article, the author(s) used Claude 3.5 Sonnet by Anthropic for the purposes of literature search assistance, initial draft organization, grammar and style refinement.
The author(s) have reviewed and edited all AI-assisted output and take full responsibility for the accuracy, integrity, and originality of the content of this publication. All medical claims have been independently verified against peer-reviewed sources by the designated medical reviewer.
In accordance with ICMJE and COPE guidelines, AI tools are not listed as authors as they cannot take accountability for the work. This disclosure follows FTC transparency requirements for digital content.
⚕️ Medical Disclaimer: This article is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay seeking it because of something you have read on this website.