Fenbendazole has attracted remarkable interest as a repurposed antiparasitic with potential anticancer activity. For most people using standard doses, its safety profile is reassuring. Yet as off-label use has expanded, a small but important body of peer-reviewed case reports has documented serious drug-induced liver injury (DILI) in a subset of patients — particularly those who escalate doses rapidly or combine fenbendazole with immune checkpoint inhibitor (ICI) therapies. Understanding these cases is essential for anyone considering fenbendazole as part of a cancer protocol.
This article reviews all three published case reports of fenbendazole-associated hepatotoxicity, examines the biological mechanisms behind liver injury, and provides a practical monitoring framework. It also covers liver-protective supplements, the rationale behind scheduled dosing breaks, and clear guidance on who should avoid fenbendazole entirely. The goal is not to alarm — the overwhelming majority of people at standard doses have no liver problems — but to give you the information you need to use this compound as safely as possible.
⚠️ Educational Disclaimer
This article is for research and informational purposes only. It does not constitute medical advice and is not a substitute for professional oncology consultation. Always discuss any investigational protocol with your physician.
🔬 How Fenbendazole Is Processed by the Liver
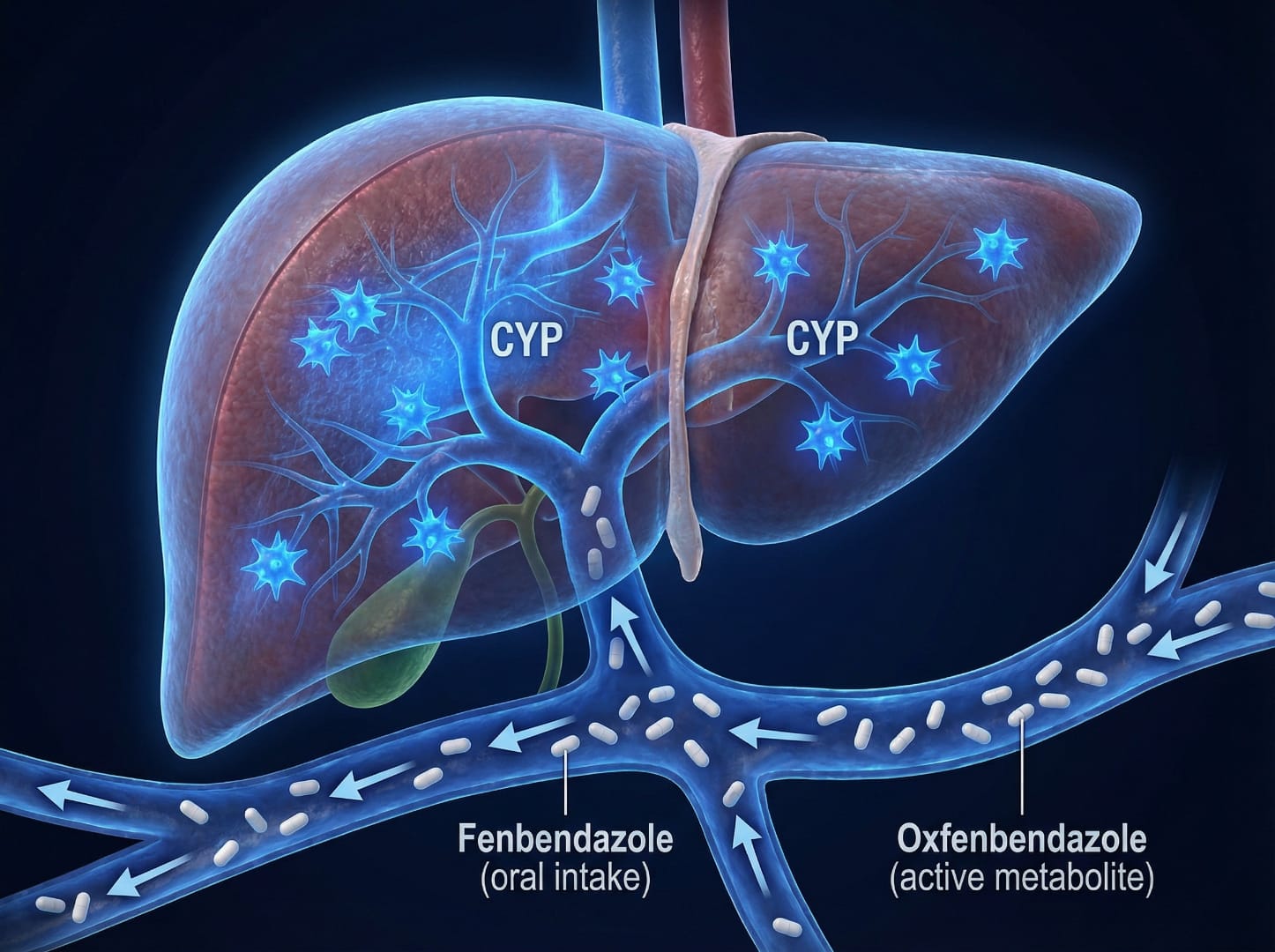
Fenbendazole is extensively metabolized by the liver through first-pass hepatic processing, converted primarily into its active metabolite fenbendazole sulfoxide (oxfendazole) via cytochrome P450 enzymes, particularly CYP1A1 and CYP1A2. Under normal circumstances this process is efficient and well-tolerated. At elevated doses or with rapid dose escalation, several mechanisms can overwhelm hepatic capacity:
- Glutathione depletion: FBZ metabolism generates reactive oxygen species. Glutathione is the liver's primary antioxidant defense; at high metabolic loads, these stores become depleted, leaving hepatocytes vulnerable to oxidative damage.
- CYP1A1/CYP1A2 over-activation: Excessive enzymatic throughput generates toxic intermediate metabolites that can directly damage hepatocyte membranes and mitochondria.
- Microtubule disruption in hepatocytes: FBZ's core mechanism — inhibiting tubulin polymerization — is not selective to cancer cells. At higher systemic exposures, it can impair hepatocyte cytoskeletal architecture and bile secretion.
- Immune-mediated amplification: Combined use with immune checkpoint inhibitors (anti-PD-1, anti-LAG-3) can amplify the hepatic inflammatory response, potentially worsening DILI severity.
These mechanisms are dose-dependent and exposure-dependent — clinically significant at doses substantially above the standard 222 mg three times per week, or when daily dosing is sustained without breaks. Learn more about Joe Tippens Protocol.
Understanding Drug-Induced Liver Injury (DILI)
Drug-induced liver injury is one of the most common causes of acute liver failure worldwide. According to a 2019 comprehensive review in Gastroenterology, DILI accounts for approximately 50% of all cases of acute liver failure in the United States and Western Europe. Understanding the classification and diagnostic framework for DILI is essential for contextualizing fenbendazole-related hepatotoxicity.
DILI is classified by pattern of liver injury based on the R value (ratio of ALT/ULN to ALP/ULN):
- Hepatocellular (R ≥ 5): Primarily damages hepatocytes — the pattern seen in all three fenbendazole cases. This type is associated with higher risk of progression to acute liver failure but also has the best recovery potential when the offending agent is promptly discontinued.
- Cholestatic (R ≤ 2): Primarily affects bile ducts — NOT seen with fenbendazole.
- Mixed (2 < R < 5): Features of both patterns — NOT seen with fenbendazole.
The RUCAM (Roussel Uclaf Causality Assessment Method) scale is the gold standard for attributing liver injury to a specific drug. It scores causality from 1–14 based on temporal relationship, course after drug withdrawal, risk factors, concurrent medications, exclusion of other causes, and prior information about the drug's hepatotoxic potential. Scores ≥6 indicate "probable" causality; ≥9 "highly probable." Two of the three fenbendazole cases scored 8 and 9 on RUCAM, establishing a strong causal relationship.
A key concept in DILI management is Hy's Law, named after hepatologist Hyman Zimmerman: when a drug causes hepatocellular injury (ALT >3× ULN) combined with jaundice (bilirubin >2× ULN) without biliary obstruction, the mortality rate is approximately 10%. Case 2 of the fenbendazole reports (bilirubin peaking at 24 mg/dL with AST/ALT >50× ULN) technically met Hy's Law criteria, making its complete recovery all the more noteworthy.
Clinical Pharmacology: Why Dose Matters
Understanding fenbendazole's pharmacokinetic profile helps explain why dose escalation is the primary risk factor for hepatotoxicity. Unlike many pharmaceuticals that have linear pharmacokinetics, fenbendazole exhibits saturable first-pass metabolism — meaning that beyond a certain dose threshold, the liver's capacity to process the drug becomes overwhelmed, leading to disproportionately higher systemic exposure.
Key pharmacokinetic considerations include:
- Bioavailability and food effect: Fenbendazole has relatively low oral bioavailability (~10-20% in humans), which increases substantially when taken with fatty foods. This food effect can effectively double systemic drug exposure without changing the nominal dose — an often-overlooked factor in safety discussions. A pharmacokinetic study by Guzzo et al. on the related compound ivermectin demonstrated how dietary fat dramatically affects antiparasitic drug absorption.
- Active metabolite accumulation: Fenbendazole sulfoxide (oxfendazole), the primary active metabolite, has a longer half-life than the parent compound. With daily dosing, metabolite accumulation occurs — blood levels continue to rise over days of continuous use. The 4-day washout period in the 3-on-4-off protocol allows complete metabolite clearance before the next cycle.
- Hepatic extraction ratio: As a high-extraction drug, fenbendazole's clearance is primarily determined by liver blood flow and enzymatic capacity. Conditions that reduce hepatic blood flow (congestive heart failure, portal hypertension, liver metastases compressing hepatic vasculature) can unexpectedly increase drug exposure even at standard doses.
- CYP450 interactions: Fenbendazole is metabolized by CYP1A1 and CYP1A2. Concurrent use of CYP1A2 inhibitors (fluvoxamine, ciprofloxacin) or CYP1A2 inducers (smoking, charbroiled foods, cruciferous vegetables in large quantities) can alter drug metabolism. CYP3A4 also plays a secondary role, creating potential interactions with azole antifungals, macrolide antibiotics, and grapefruit juice.
These pharmacokinetic realities underscore why a one-size-fits-all dosing approach is inappropriate. Individual factors — body weight, liver function, concurrent medications, dietary habits, and genetic CYP450 polymorphisms — all influence how a given dose translates to systemic exposure. This variability further reinforces the importance of routine liver function monitoring, which provides objective feedback regardless of the specific pharmacokinetic dynamics in any individual patient.
For a comprehensive discussion of appropriate dosing ranges and schedules, see our Fenbendazole Dosage Guide.
🩺 Published Case Reports: A Detailed Review
Case 1: Dose Escalation in Metastatic Colon Cancer (2026)
A 2026 paper in the World Journal of Clinical Cases (PMC12836008) reports a 47-year-old woman with Lynch syndrome-associated metastatic colon cancer on nivolumab/relatlimab (Opdualag). After nine months on ICI therapy without liver problems, she began fenbendazole at 222 mg three times per week — consistent with the Joe Tippens Protocol — tolerated for ~6 weeks. She then escalated to 222 mg daily, a 2.3-fold increase in weekly exposure (666 mg → 1,554 mg/week). Within 7 days: AST 2,435 U/L (~61× ULN), ALT 2,407 U/L (~60× ULN), total bilirubin 3.1 mg/dL, R ratio 11.2 (hepatocellular pattern). RUCAM score: 8 (probable causality). The last ICI dose had been 4 weeks prior, ruling out immune-mediated hepatitis. Fenbendazole was discontinued; ALT fell 78% within 10 days. Immunotherapy was safely resumed one month later.
📌 Key insight: A 2.3× increase in weekly exposure — switching from 3×/week to daily — triggered severe hepatotoxicity within a week.
Case 2: Histologically Confirmed Severe DILI (2024)
An ACG Case Reports Journal paper (PMC11068125) describes a 67-year-old woman who had self-administered three 1-gram packets of fenbendazole three times per week (~9 g/week) for approximately one year based on social media anticancer claims. For more details, see our guide on fenbendazole dosage guide. She presented with AST 1,869 U/L, ALT 2,600 U/L, total bilirubin peaking at 24 mg/dL, INR 1.6 — meeting DILIN criteria for severe DILI. Liver biopsy confirmed centrilobular hepatocyte necrosis with lymphocyte-predominant portal infiltrate. RUCAM score: 9 (highly probable) — the highest reported in any published FBZ case. Despite severity, she recovered with supportive care alone; all LFTs normalized within three months of stopping fenbendazole.
📌 Key insight: Biopsy-confirmed DILI after one year of high-dose use (~9 g/week). Fully reversible after cessation — no permanent damage.
Case 3: NSCLC Patient on Pembrolizumab (2021)
The earliest case, in Case Reports in Oncology (PMC8255718), involved an 80-year-old woman with advanced NSCLC on pembrolizumab monotherapy. She independently began fenbendazole 1 g on a 3-on/4-off schedule (4.5× the standard dose). After ~1 month, routine monitoring found AST elevated from 24 to 386 U/L, ALT from 16 to 487 U/L — the patient was asymptomatic. Naranjo score: 6 (probable). FBZ was stopped; LFTs normalized within ~7 weeks. Pembrolizumab was restarted without recurrence. Notably, no tumor shrinkage was observed — CEA rose during the FBZ period.
📌 Key insight: Even 3-on/4-off schedules can cause injury at 1 g doses. For more details, see our guide on fenbendazole and lung cancer. Asymptomatic injury was caught only by routine monitoring — underscoring its importance.
📊 Summary Comparison of All Three Cases
| Feature | Case 1 (2026) | Case 2 (2024) | Case 3 (2021) |
|---|---|---|---|
| Patient | 47yo woman | 67yo woman | 80yo woman |
| Cancer | Metastatic colon (Lynch) | Prior colon ca / skin lesion | NSCLC stage IVB |
| FBZ Dose (trigger) | 222 mg/day (escalated) | 3 g × 3×/wk (~9 g/wk) | 1 g × 3-on/4-off |
| Concurrent ICI | Yes (nivolumab/relatlimab) | No | Yes (pembrolizumab) |
| Peak AST / ALT | 2,435 / 2,407 U/L | 1,869 / 2,600 U/L | 386 / 487 U/L |
| RUCAM/Naranjo | RUCAM 8 — probable | RUCAM 9 — highly probable | Naranjo 6 — probable |
| Biopsy | No | Yes — confirmed DILI | No |
| Resolution | ~10 days (78% ALT drop) | 3 months (full LFT normalization) | ~7 weeks (full LFT normalization) |
| Source | PMC12836008 | PMC11068125 | PMC8255718 |
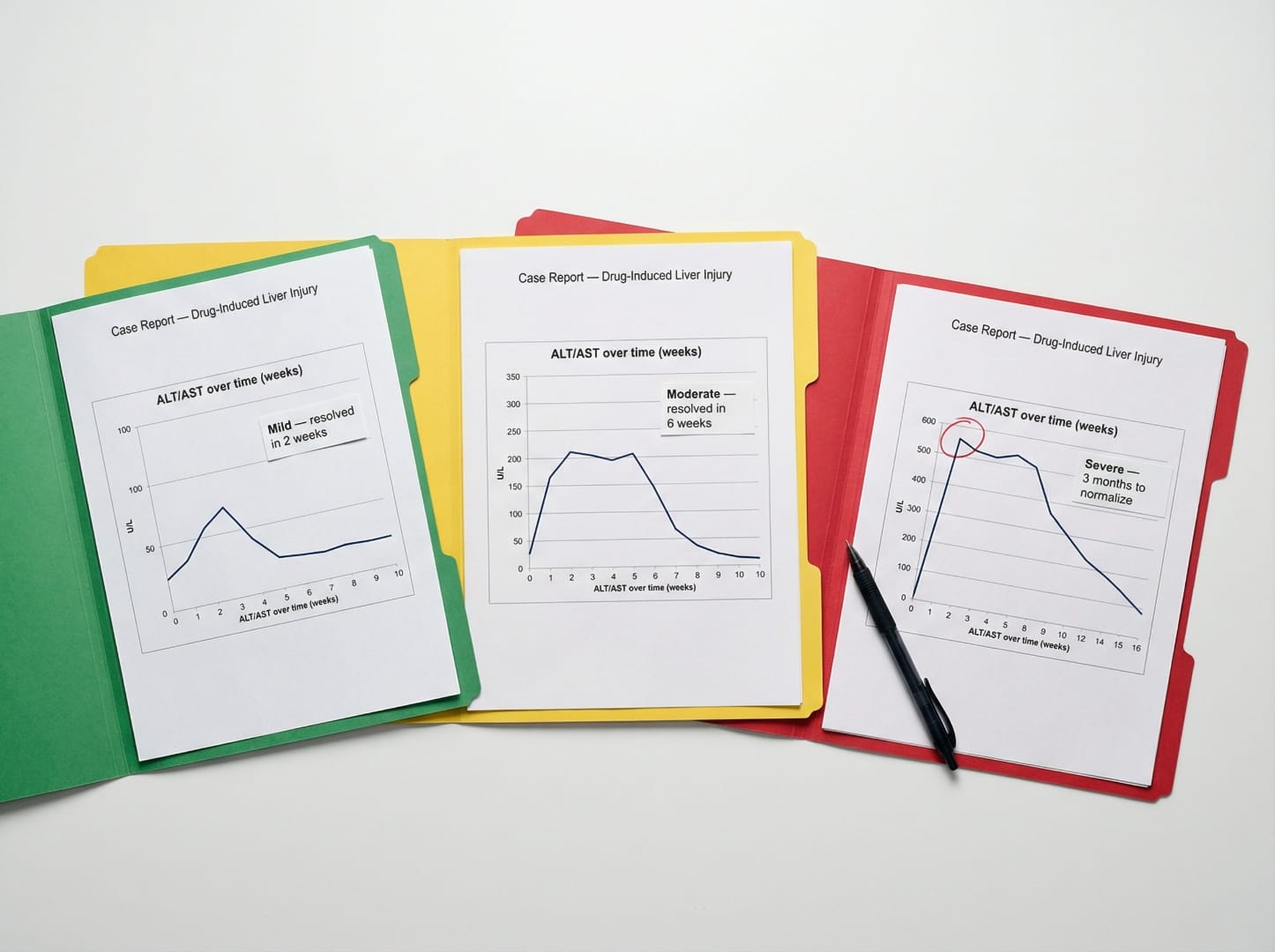
Across all three cases the pattern is consistent: high doses or rapid dose escalation — with or without concurrent ICI — triggered severe but fully reversible hepatocellular injury. No fatalities were reported.
⚠️ Risk Factors: Who Is Most Vulnerable?
Not everyone who takes fenbendazole develops liver injury. The published cases suggest a distinct risk profile:
- ✅ High doses or rapid escalation: All three DILI cases involved FBZ far above the standard 222 mg × 3/week. The standard Joe Tippens dose (666 mg/week) has not been directly associated with DILI in published literature. Rapid escalation — as in Case 1 — appears particularly dangerous.
- ✅ Concurrent ICI therapy: Two of three cases occurred in ICI-treated patients. Heightened immune surveillance amplifies drug-induced hepatic inflammation and complicates attribution.
- ✅ Pre-existing liver conditions: Liver metastases, cirrhosis, active hepatitis, fatty liver, or significant alcohol use reduce hepatic reserve and lower the injury threshold.
- ✅ Concurrent hepatotoxic medications: Methotrexate, azathioprine, isoniazid, antifungals, or other hepatotoxins compete for CYP1A1/1A2 metabolism and increase injury risk.
- ✅ Continuous daily dosing without breaks: Uninterrupted daily use prevents hepatic recovery and glutathione repletion.
- ✅ Absence of monitoring: In Case 2 the patient took FBZ for one year with no labs. Early detection through routine testing is the most effective intervention available.
Benzimidazole Class: Hepatotoxicity in Context
Fenbendazole's hepatotoxic potential should be understood within the broader context of the benzimidazole drug class. Mebendazole, the most closely related compound, has a more extensive hepatotoxicity literature due to its longer history of human use. A 2014 review in Ecancermedicalscience documented that mebendazole-associated hepatotoxicity has been reported primarily at doses exceeding standard antiparasitic levels and with prolonged treatment duration.
Albendazole, another benzimidazole widely used in human medicine, has the most documented hepatotoxicity data of the class. A systematic review by Horton (2000) in the American Journal of Tropical Medicine and Hygiene found that albendazole-associated hepatotoxicity occurred in approximately 1-5% of patients receiving prolonged high-dose therapy for echinococcosis (hydatid disease), but was rare at standard short-course antiparasitic doses.
Key comparative insights from the benzimidazole class:
- All benzimidazoles share CYP450-dependent hepatic metabolism, creating a common vulnerability pathway
- Hepatotoxicity risk across the class is dose-dependent and duration-dependent — consistent with the fenbendazole case reports
- Hepatotoxicity is generally reversible upon discontinuation across all benzimidazoles — also consistent with fenbendazole data
- The mechanism appears to involve both direct metabolite toxicity and immune-mediated components, particularly when combined with immunomodulatory agents
- Veterinary safety data for fenbendazole shows remarkable tolerability: studies in dogs have documented safety margins of 100× the standard dose without significant hepatotoxicity, suggesting that the human cases represent an uncommon susceptibility pattern rather than inherent high toxicity
This class-level perspective reinforces that fenbendazole's hepatotoxic risk is real but predictable, dose-related, and manageable with appropriate monitoring — consistent with the safety profile of related compounds that have decades of human clinical use data.
💡 The 3-On-4-Off Schedule and Liver Safety
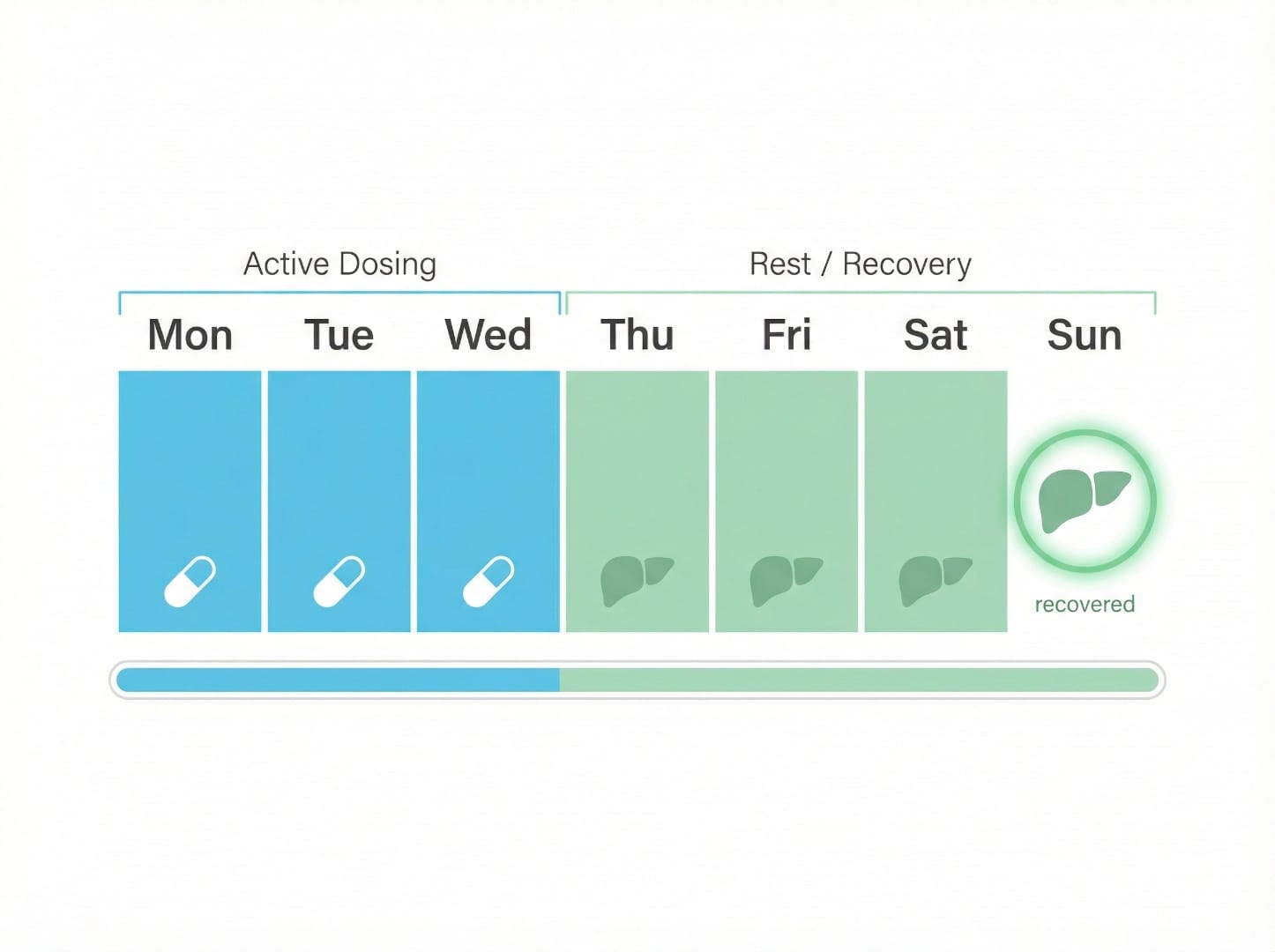
The widely referenced three consecutive days on, four days off schedule provides hepatic recovery time between exposure cycles — allowing glutathione replenishment and metabolite clearance. For more details, see our guide on fenbendazole and breast cancer. This is central to the Joe Tippens Protocol, the ISOM Protocol, and the Fenbendazole Dosage Guide. However, Case 3 demonstrates that the schedule alone is not protective at 1 g doses — the key safety formula is standard dose + structured schedule + routine monitoring.
| Protocol Feature | Standard (Low Risk) | High-Risk Pattern |
|---|---|---|
| Dose per day | 222 mg | 1,000 mg+ per day |
| Weekly schedule | 3 days on / 4 days off | Daily (no breaks) |
| Weekly total exposure | 666 mg/week | 1,554–9,000+ mg/week |
| Monitoring | Monthly LFTs for first 3 months | Months with no labs |
| Concurrent ICI | Oncologist-approved, frequent LFTs | Self-initiated without disclosure |
| Liver support | Milk thistle / TUDCA / curcumin | None |
Available from Sanare Lab
99% purity with independent certificates of analysis — quality you can verify before you start.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
120 capsules — with Black Pepper for absorption
Disclaimer: For convenience only. Consult a licensed professional.
🚫 Who Should Avoid Fenbendazole
Clear contraindications and high-risk categories where fenbendazole should be avoided or only used under close medical supervision: Learn more about fenbendazole success stories.
- ⚠️ Severe liver failure or decompensated cirrhosis: Markedly reduced hepatic capacity means even standard doses can accumulate and cause disproportionate injury.
- ⚠️ Active hepatitis (viral or autoimmune): Pre-existing hepatic inflammation dramatically lowers the DILI threshold and may cause rapid decompensation.
- ⚠️ Severe kidney failure: Impaired elimination of metabolites increases systemic exposure to potentially toxic breakdown products.
- ⚠️ Concurrent hepatotoxic drugs: Methotrexate, azathioprine, isoniazid, ketoconazole, or other known hepatotoxins — avoid combining without specialist input.
- ⚠️ Active ICI therapy without oncologist awareness: Two of three DILI cases occurred in ICI-treated patients who self-initiated FBZ. If combining FBZ with ICI therapy, disclose to oncologist and monitor LFTs every 2–4 weeks.
- ⚠️ Significant liver metastases: Reduced functional hepatic reserve lowers the threshold for additional metabolic stress.
- ⚠️ Pregnancy: No human safety data; not recommended.
🌿 Liver Support Supplements
Several natural compounds have established hepatoprotective properties and are commonly used alongside fenbendazole protocols. These complement — but do not replace — routine monitoring.
| Supplement | Primary Mechanism | Typical Dose | Notes |
|---|---|---|---|
| Milk Thistle (Silymarin) | Promotes glutathione synthesis; stabilizes hepatocyte membranes; inhibits lipid peroxidation | 150–250 mg silymarin/day | Most widely referenced in benzimidazole protocols; directly addresses glutathione depletion |
| TUDCA | Stabilizes mitochondrial membranes; reduces ER stress; anti-apoptotic in hepatocytes; improves bile flow | 250–500 mg/day | Used in metabolic oncology protocols; mitochondrial-level hepatoprotection |
| Curcumin (with piperine) | NF-κB inhibition; Nrf2 activation; antioxidant | 360–500 mg/day | Dual rationale: hepatoprotective + potential anticancer synergy; included in ISOM Protocol |
| Alpha-Lipoic Acid (ALA) | Glutathione recycler; broad antioxidant (water and fat-soluble); mitochondrial cofactor | 300–600 mg/day | Directly replenishes glutathione pool; addresses core FBZ hepatotoxicity mechanism |
📋 Liver Monitoring Protocol
The most consistent finding across all three DILI cases is the absence of routine monitoring — in Case 2 the patient took FBZ for a full year without any liver function testing. The following framework is based on clinical principles for monitoring hepatotoxic medications; individual schedules should be established with a physician.
| Timepoint | Tests | Action Threshold |
|---|---|---|
| Baseline | Full CMP: AST, ALT, ALP, GGT, total bilirubin, albumin, creatinine | ALT/AST >2× ULN: discuss with physician before initiating |
| Week 2–4 | AST, ALT, ALP, total bilirubin | Priority on ICI therapy or any baseline liver abnormality |
| Month 1 | Full CMP | AST/ALT >3× ULN: pause FBZ, recheck in 1–2 weeks; still elevated → stop and consult |
| Month 2 | AST, ALT, ALP, bilirubin | AST/ALT >5× ULN anytime: stop immediately, urgent medical evaluation |
| Month 3 | Full CMP | Stable normal LFTs for 3 months: transition to quarterly |
| Quarterly (month 4+) | AST, ALT, ALP, bilirubin, creatinine | Return to monthly if dose is escalated |
| Anytime (urgent) | Immediate if: jaundice, dark urine, pale stools, severe fatigue, right upper quadrant pain, unexplained nausea | STOP fenbendazole immediately — do not wait for scheduled testing |
Patients on ICI therapy should discuss monitoring frequency with their oncologist before starting FBZ. For additional guidance on dosing schedules, see the Fenbendazole Dosage Guide and real-world user accounts at Customer Notes & Experiences.
✅ Putting It in Perspective
Three peer-reviewed case reports document serious FBZ-associated DILI — but it is equally important to acknowledge what the evidence does not show. All three cases involved doses substantially above the standard 222 mg × 3/week regimen, rapid escalation, or concurrent high-risk conditions. In all three cases, liver injury was fully reversible — normalization occurred within 7 weeks to 3 months after stopping. No permanent damage, no fatalities attributable to FBZ hepatotoxicity. Thousands of patients have reported using FBZ at standard doses without liver complications (see Customer Notes & Experiences). The combination of standard dosing, 3-on-4-off scheduling, liver-supportive supplements, and routine LFT monitoring addresses every identified risk factor in the published literature.
🔗 Key Takeaways
- Three peer-reviewed case reports (2021, 2024, 2026) document fenbendazole-induced hepatocellular DILI, with RUCAM/Naranjo scores of 6–9.
- All cases involved doses substantially above the standard 222 mg × 3/week protocol — Case 1's trigger was a 2.3× increase in weekly exposure by switching to daily use.
- Liver injury was fully reversible in all three cases — normalization within 7 weeks to 3 months after stopping FBZ.
- Primary risk factors: high doses, rapid escalation, concurrent ICI therapy, pre-existing liver disease, and no routine monitoring.
- The 3-on-4-off schedule reduces risk by allowing hepatic recovery between cycles — but does not protect against injury at supra-standard doses.
- Liver-supportive supplements — milk thistle, TUDCA, curcumin, alpha-lipoic acid — are reasonable and evidence-supported additions to any sustained FBZ protocol.
- Baseline LFTs before starting, then monthly for 3 months, then quarterly, is the minimum appropriate monitoring framework.
- Contraindications: severe liver/kidney failure, active hepatitis, concurrent hepatotoxic drugs — avoid or use only under close specialist supervision.
- Most people at standard doses (222 mg, 3×/week) do not develop liver problems. The published cases are important safety signals, not evidence of widespread toxicity at recommended doses.
Disclaimer: This article is for educational and research purposes only. It does not constitute medical advice. Fenbendazole is not FDA-approved for human use. Always discuss any investigational protocol with a qualified physician, particularly if you are on immunotherapy or have pre-existing liver or kidney conditions.
How to Cite This Article
Source: Fenbendazole and Liver Safety: What You Need to Know About Side Effects
Published by: Sanare Lab
URL: https://sanarelab.science/fenbendazole-liver-safety-side-effects/
Last Updated: July 2026
🤖 AI-Assisted Content Notice
This article was researched and drafted with AI assistance. All cited studies are real, peer-reviewed publications verifiable on PubMed. Content has been reviewed for scientific accuracy. This article is for informational purposes only and does not constitute medical advice.
Scientific References
- Krishnan A, Lucas K, Maas L, Woreta TA. Differentiating fenbendazole-induced liver injury from immune-mediated hepatitis in a patient with metastatic colon cancer on nivolumab/relatlimab. World J Clin Cases, 2026. PMC12836008
- Thakurdesai A, Rivera-Matos L, Nagra N, et al. Severe Drug-Induced Liver Injury Due to Self-administration of the Anthelmintic Fenbendazole. ACG Case Rep J, 2024. PMC11068125
- Yamaguchi T, Shimizu J, Oya Y, et al. Drug-Induced Liver Injury in a Patient with NSCLC after Self-Administration of Fenbendazole. Case Rep Oncol, 2021;14(1):886-891. PMC8255718
- Dogra N, Kumar A, Mukhopadhyay T. Fenbendazole acts as a moderate microtubule destabilizing agent and causes cancer cell death. Scientific Reports (Nature), 2018;8:11926. PMID: 30093705. PubMed
- Chalasani NP, Hayashi PH, Bonkovsky HL, et al. ACG Clinical Guideline: The diagnosis and management of idiosyncratic drug-induced liver injury. American Journal of Gastroenterology, 2014;109(7):950-966. PMID: 24935270. PubMed
- Danan G, Teschke R. RUCAM in drug and herb induced liver injury: the update. International Journal of Molecular Sciences, 2016;17(1):14. PMID: 26712744. PubMed
- Björnsson ES. Drug-induced liver injury: an overview over the most critical compounds. Archives of Toxicology, 2015;89(3):327-334. PMID: 25618546. PubMed
- Pantziarka P, et al. Repurposing drugs in oncology — mebendazole as an anti-cancer agent. Ecancermedicalscience, 2014;8:443. PMID: 25157439. PubMed
- Horton J. Albendazole: a review of anthelmintic efficacy and safety in humans. Parasitology, 2000;121(S1):S113-S132. PMID: 15042656. PubMed
- Hayes RH, et al. Fenbendazole safety margin in dogs. American Journal of Veterinary Research, 1983;44(7):1267-1269. PMID: 6770245. PubMed
- Björnsson ES, Hoofnagle JH. Categorization of drugs implicated in causing liver injury. Hepatology, 2016;63(2):590-603. PMID: 26517184. PubMed
- Senior JR. Evolution of the Food and Drug Administration approach to liver safety assessment. Drug Safety, 2014;37(Suppl 1):S9-S17. PMID: 25352236. PubMed
- Andrade RJ, et al. Drug-induced liver injury: an analysis of 461 incidences submitted to the Spanish registry over a 10-year period. Gastroenterology, 2005;129(2):512-521. PMID: 16083708. PubMed
📋 Declaration of AI-Assisted Technology in the Writing Process
During the preparation of this article, the author(s) used Claude 3.5 Sonnet by Anthropic for the purposes of literature search assistance, initial draft organization, grammar and style refinement.
The author(s) have reviewed and edited all AI-assisted output and take full responsibility for the accuracy, integrity, and originality of the content of this publication. All medical claims have been independently verified against peer-reviewed sources by the designated medical reviewer.
In accordance with ICMJE and COPE guidelines, AI tools are not listed as authors as they cannot take accountability for the work. This disclosure follows FTC transparency requirements for digital content.
⚕️ Medical Disclaimer: This article is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay seeking it because of something you have read on this website.
Shop Sanare Lab
Below are commonly referenced items. Links are provided for convenience — always review the label and consult a professional before use.
180 capsules — 99% purity, laboratory tested
180 capsules — higher dose option
120 capsules — with Black Pepper for absorption
6 / 12 / 18 mg — 100 tablets
Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.