Turmeric & Curcumin for Cancer: What Human and Preclinical Research Shows
Curcumin's anti-cancer mechanisms in human trials and preclinical research. Bioavailability challenges, optimal formulations, and combination protocols with other compounds.

This article is for research and informational purposes only. It does not constitute medical advice. Do not self-prescribe. Always consult a qualified healthcare provider before using any supplement, especially alongside cancer treatment.
Table of Contents
- Cancer burden and the search for better-tolerated strategies
- Turmeric for Cancer vs. Curcumin
- How curcumin affects cancer cells in laboratory models
- Specific cancer types: what does the preclinical data say?
- Key Molecular Mechanisms Explained
- Bioavailability: the critical challenge
- Why formulations matter: phytosomes, piperine, and nanoparticles
- What do human clinical trials show?
- Curcumin + chemotherapy: synergy data
- Curcumin and immunotherapy
- Oral cancer: a Phase II breakthrough
- Curcumin and Cancer Stem Cells
- Epigenetic Effects: How Curcumin May Reprogram Gene Expression
- Endoplasmic Reticulum Stress, Autophagy and Apoptosis
- Additional Cancer Types: Ovarian, Cervical, Gastric, Bladder and Melanoma
- Curcumin and Radiation Therapy: Radiosensitization and Radioprotection
- Curcumin Analogs: EF24, BDMC and the Next Generation
- Nanoparticle Delivery: Closing the Bioavailability Gap
- What the Meta-Analyses Actually Conclude (2024–2026)
- Safety Profile and Drug Interactions
- Curcumin and Fenbendazole: What the Evidence Actually Shows
- What this means for informed consumers
- Bottom line
- Frequently Asked Questions
- References
Cancer burden and the search for better-tolerated strategies
Cancer remains the second leading cause of death globally. In 2020 alone, approximately 18.1 million new cancer cases and nearly 10 million cancer-related deaths were reported worldwide. Projections suggest global cancer incidence could increase by 31–47% by 2030–2040, depending on region and cancer type.
While conventional treatments such as chemotherapy, radiation, and targeted therapies have improved survival in many cancers, they are often limited by toxicity, resistance, and long-term side effects. This has driven growing scientific interest in adjunct compounds that may modulate cancer-related pathways with lower toxicity profiles — including curcumin.
Turmeric for Cancer vs. Curcumin: What You Actually Need to Know
Turmeric (Curcuma longa) has been used in Ayurvedic and traditional Chinese medicine for more than 4,000 years. Modern research attributes most of turmeric's pharmacological activity to curcuminoids — primarily curcumin, demethoxycurcumin, and bisdemethoxycurcumin. Of these, curcumin has received the most scientific attention as a potential anticancer agent.
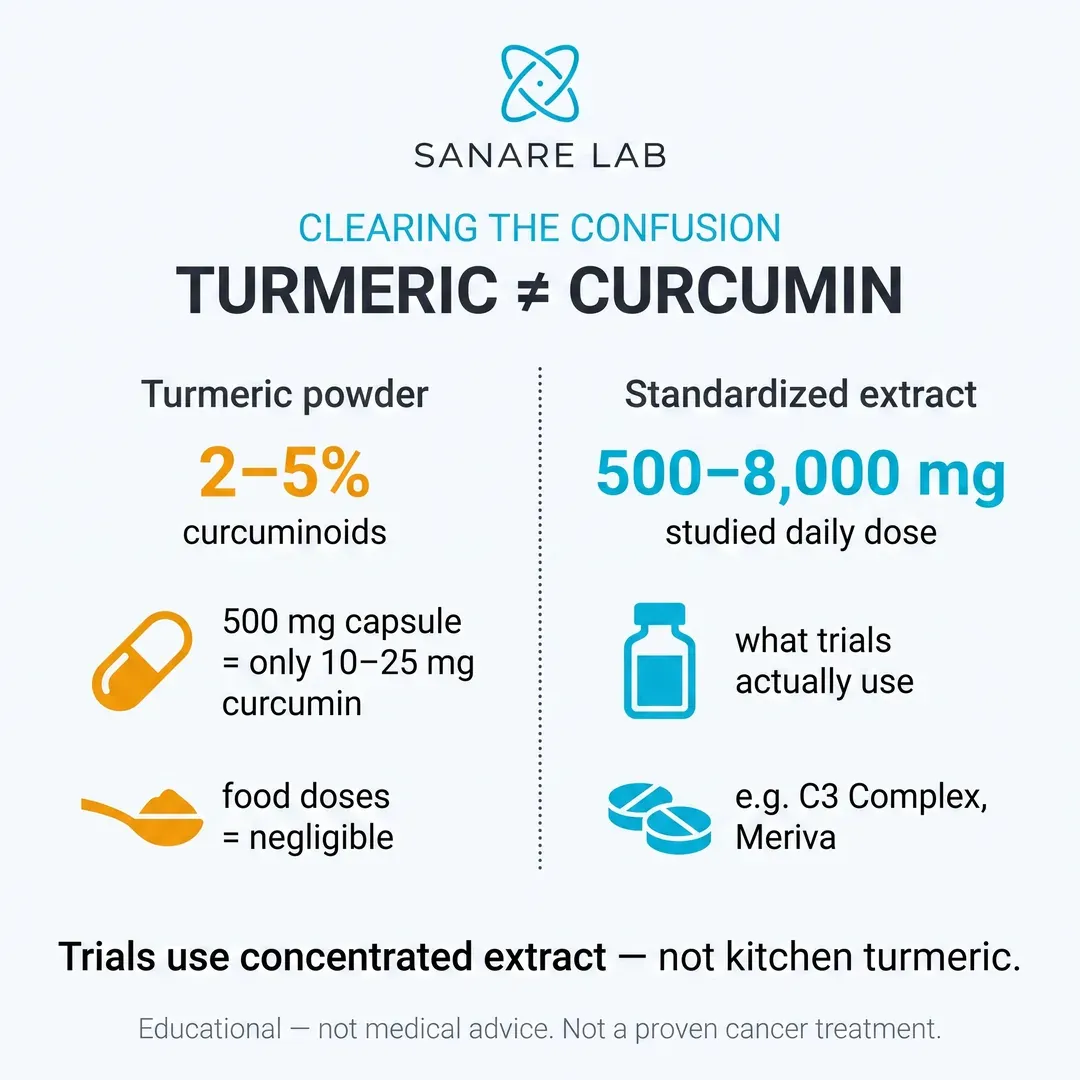
A common source of confusion is the difference between turmeric supplements and curcumin extracts. Whole turmeric powder contains only 2–5% curcuminoids, meaning a typical 500 mg turmeric capsule delivers just 10–25 mg of curcumin — far below the doses used in clinical trials (500–8,000 mg/day of standardized curcumin). This is why researchers and oncology-focused protocols such as the Joe Tippens Protocol specify standardized curcumin extracts (e.g., Curcumin C3 Complex or Meriva phytosome), not raw turmeric powder.
For consumers searching "turmeric for cancer," the practical takeaway is: dietary turmeric in food (curries, golden milk) contributes negligible curcumin for any pharmacological effect. To match the dosing studied in human trials, a bioavailability-enhanced curcumin supplement is necessary — and even then, curcumin remains an investigational compound, not a proven cancer treatment.
How curcumin affects cancer cells in laboratory models
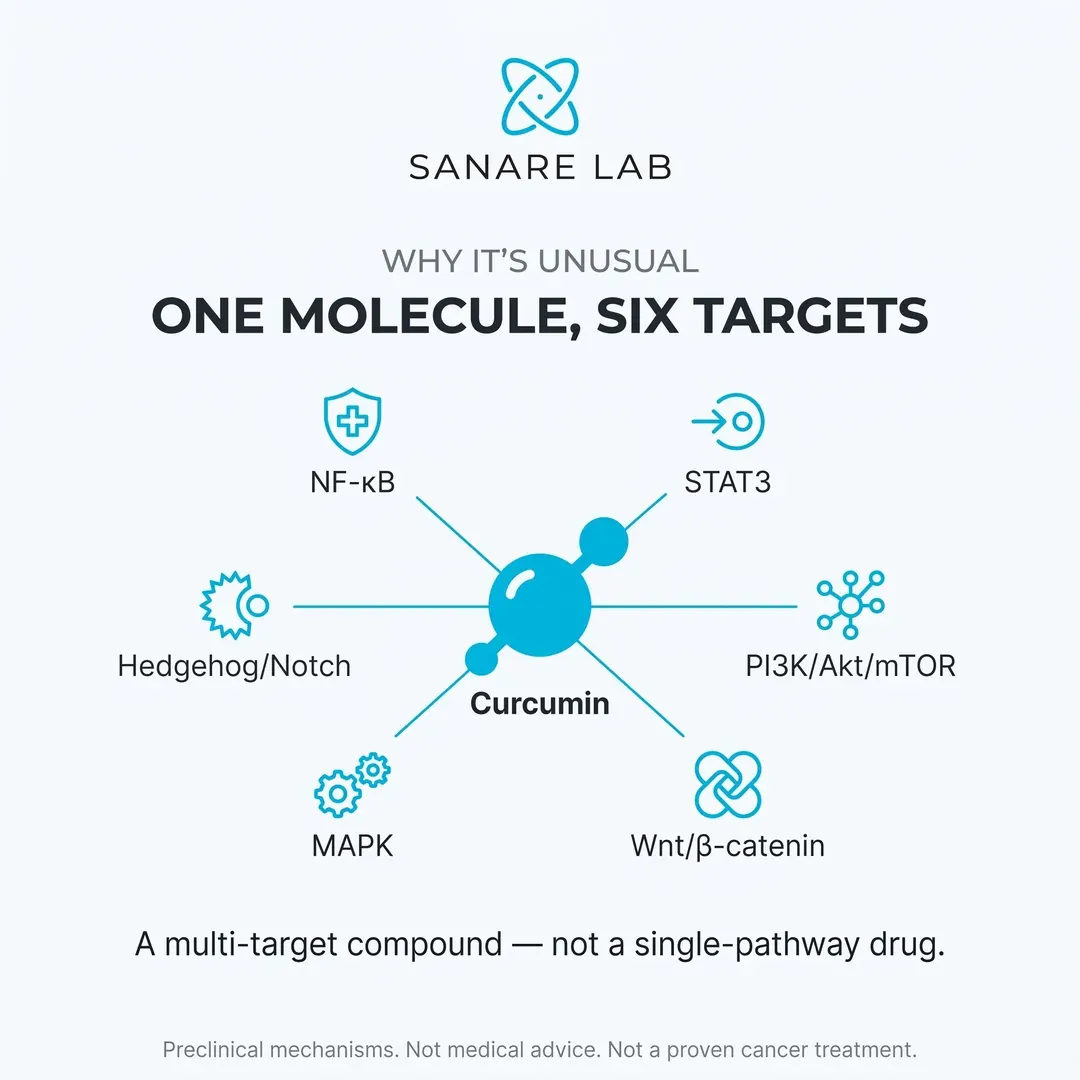
According to the 2024 review, curcumin demonstrates anti-proliferative and pro-apoptotic effects across a wide range of cancer cell lines in laboratory and animal models. These effects are not limited to a single mechanism — curcumin simultaneously targets multiple pathways that are commonly dysregulated in cancer:
By modulating all these pathways simultaneously, curcumin has been shown in experimental models to reduce cancer cell proliferation, induce programmed cell death (apoptosis), inhibit angiogenesis, and suppress invasion and metastasis-related signaling.
Importantly, curcumin acts as a multi-target compound, rather than a single-pathway inhibitor — a property that may explain its broad biological activity in preclinical research. This is what distinguishes it from most single-target pharmaceutical agents.
Specific cancer types: what does the preclinical data say?
Curcumin has been studied across a remarkably wide range of cancer types. For more details, see our guide on Joe Tippens Protocol. Here is a summary of key findings from recent reviews:
A 2025 study from Frontiers in Oncology identified a new mechanism in colorectal cancer: curcumin directly binds to and inhibits CDK2, disrupting the CDK2–c-MYC–PTBP1 regulatory axis. In xenograft mouse models, curcumin at 100 mg/kg daily significantly reduced tumor volumes and decreased tumor cell density with no visible signs of systemic toxicity.
Key Molecular Mechanisms Explained
Consolidated from a previous standalone mechanisms overview to eliminate keyword cannibalization.
STAT3 and NF-κB: central molecular targets
Two of the most extensively studied targets of curcumin are the transcription factors STAT3 and NF-κB.
STAT3 is frequently constitutively activated in many cancers, including breast, prostate, colorectal, lung, ovarian, pancreatic, and hematologic malignancies. Persistent STAT3 activation promotes tumor growth by increasing expression of genes involved in cell survival (such as Bcl-xL), proliferation (cyclin D1), angiogenesis, and immune evasion.
NF-κB plays a central role in inflammation-driven carcinogenesis and has been linked to resistance against apoptosis and chemotherapy. For more details, see our guide on Joe Tippens Protocol. Experimental studies show that curcumin can suppress both STAT3 and NF-κB signaling, leading to reduced tumor cell proliferation and increased programmed cell death in multiple cancer cell lines.
A 2024 narrative review in Frontiers in Pharmacology confirmed that curcumin and its analogues target STAT3 activation across multiple cancer types, reinforcing its relevance as a multi-pathway modulator in oncology research (PMC11680487).
Curcumin and specificity protein 1 (Sp1)
Another important mechanism discussed in the review involves Sp1 (Specificity Protein 1), a transcription factor overexpressed in many tumor cells compared to normal tissue.
Sp1 regulates several genes involved in angiogenesis, invasion, and metastasis, including VEGF, EGFR, uPA, and CD24. Research indicates that curcumin suppresses Sp1 activity and its downstream gene expression in a concentration-dependent manner, particularly in colorectal, bladder, and non-small cell lung cancer cell models.
By inhibiting Sp1, curcumin has been shown to reduce colony formation, migration, and invasive potential of cancer cells in laboratory studies.
Effects on cell adhesion and metastasis-related pathways
Curcumin also affects pathways involved in tumor invasion and metastasis. For more details, see our guide on ISOM Protocol. Experimental data suggest that curcumin inhibits focal adhesion kinase (FAK) phosphorylation while increasing expression of extracellular matrix components such as collagen, laminin, and fibronectin.
Key Takeaway: Research suggests multiple mechanisms of action including microtubule disruption, p53 pathway activation, and metabolic interference — potentially targeting cancer cells through pathways distinct from conventional chemotherapy.
Additionally, curcumin has been shown to downregulate CD24 and upregulate E-cadherin, a key molecule involved in maintaining epithelial cell integrity. These combined effects may contribute to reduced detachment, migration, and metastatic potential of cancer cells in experimental models.
Bioavailability: the critical challenge
Despite strong laboratory data, curcumin faces a critical limitation: extremely low oral bioavailability.
The numbers tell the story clearly:
- Even doses of 10–12 grams per day produce blood concentrations below 50 nanomolar
- A 2 g oral dose results in serum levels that are often undetectable by standard HPLC analysis
- Systemic bioavailability of raw curcumin is estimated at ~1% or less
- Phase I trials confirmed curcumin is safe even at 12 g/day, but bioavailability remains poor
This explains a well-known paradox: curcumin shows potent effects in cell cultures but far weaker effects in human studies when used in its unformulated (raw powder) form.
Why formulations matter: phytosomes, piperine, and nanoparticles
To address bioavailability challenges, modern research focuses heavily on curcumin delivery systems. For more details, see our guide on ISOM Protocol. The differences are dramatic:
In animal models, nano-formulated curcumin has been shown to reduce tumor size more effectively than free curcumin, sometimes within days rather than weeks, and at much lower doses. According to a 2023 ACS Omega review, the overarching goal of all strategies is to increase curcumin's solubility and bioavailability, since raw curcumin produces undetectable plasma levels even at gram-scale doses.
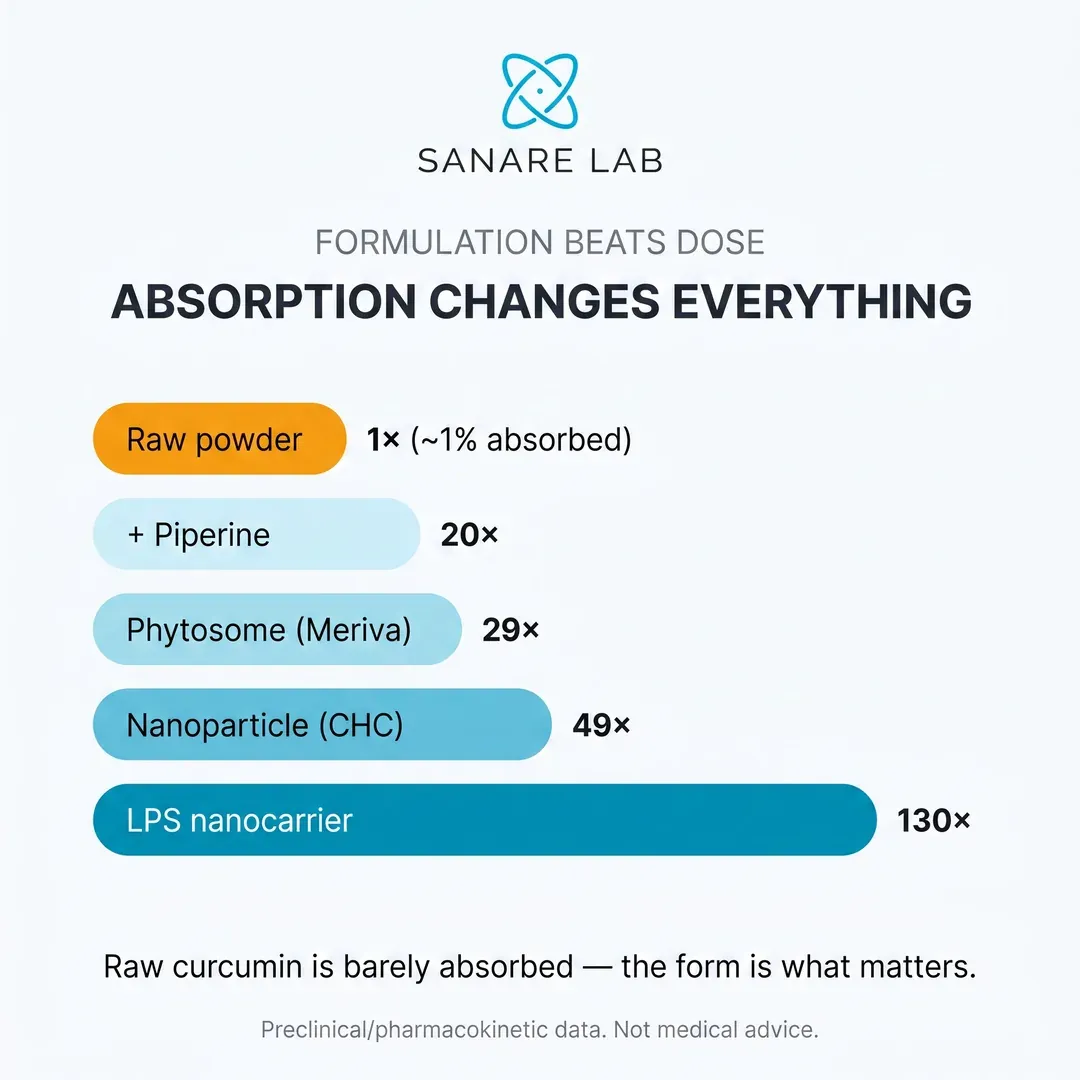
Key takeaway: Formulation quality matters far more than raw dose. A gram of phytosome curcumin delivers far more bioavailable curcumin than a gram of standard powder. When evaluating any curcumin supplement, the formulation technology is the single most important factor.
Curcumin with Enhanced Bioavailability
Below is a curcumin supplement formulated with Black Pepper extract (piperine) to enhance absorption. Link is provided for convenience — always review the label and consult a professional before use.
Curcumin Turmeric 360 mg
120 capsules — with Black Pepper & Phytosome Extract for enhanced absorption Buy Curcumin Turmeric →Disclaimer: For convenience only. This site does not provide medical advice. Consult a licensed professional.
What do human clinical trials show?
While human data remains limited compared to preclinical research, several Phase II randomized controlled trials have now produced concrete results. Here is a summary of the most significant findings:
Breast cancer — curcumin + paclitaxel (150 patients, Armenia)
A Phase II RCT gave 75 patients IV curcumin (CUC-01, 300 mg/week) alongside paclitaxel for 12 weeks. Results:
- Objective response rate at 16 weeks: 50.7% (curcumin group) vs. 33.3% (placebo) — statistically significant (p<0.05)
- At 24 weeks: 29% response in the curcumin group vs. 20% in placebo
- A separate study reported that 300 mg/day curcumin nanoparticles for 6 months produced tumor shrinkage in 60% of participants
Colorectal cancer — curcumin + FOLFOX (27 patients, UK)
A Phase IIa RCT in previously untreated Stage IV colorectal cancer patients added 2 g oral curcumin C3 complex to standard FOLFOX ± bevacizumab: Learn more about fenbendazole vs mebendazole comparison.
- 6-month overall survival (per-protocol): 93.3% (curcumin) vs. 55.6% (placebo)
- 6-month progression-free survival: 73.3% vs. 33.3%
- Median overall survival: 596 days (curcumin) vs. 200 days (placebo)
- Objective response at 12 cycles: 53.3% vs. 11.1%
Prostate cancer — curcumin during ADT withdrawal (97 patients, South Korea)
Patients with Stage IV prostate cancer received 1,440 mg/day curcumin for 6 months during androgen deprivation therapy (ADT) withdrawal. The results showed:
- PSA progression at 6 months: 10.3% (curcumin) vs. 30.2% (placebo)
- Adverse events: 15.6% (curcumin) vs. 34.8% (placebo) — curcumin was better tolerated
A separate radiation therapy study in 180 prostate cancer patients found that 3 g/day curcumin markedly reduced PSA levels and decreased radiation-related side effects (inflammation, urological complications) over 3 months.
Multiple myeloma — curcumin + MP regimen (33 patients, Indonesia)
A pilot RCT combined BCM-95 CG curcumin (8 g/day) with melphalan and prednisone. Among patients who completed the 4-month follow-up:
- Remission rate: 75% (curcumin group) vs. 33.3% (placebo)
Oral leukoplakia — curcumin alone (223 patients, India)
A Phase IIb RCT tested 3.6 g/day BCM-95 CG curcumin for 6 months in patients with confirmed oral leukoplakia (a pre-cancerous condition):
- Clinical response: 67.5% (curcumin) vs. 55.3% (placebo)
- Combined clinical + histologic response: 58% vs. 44.6%
Summary of clinical trial data
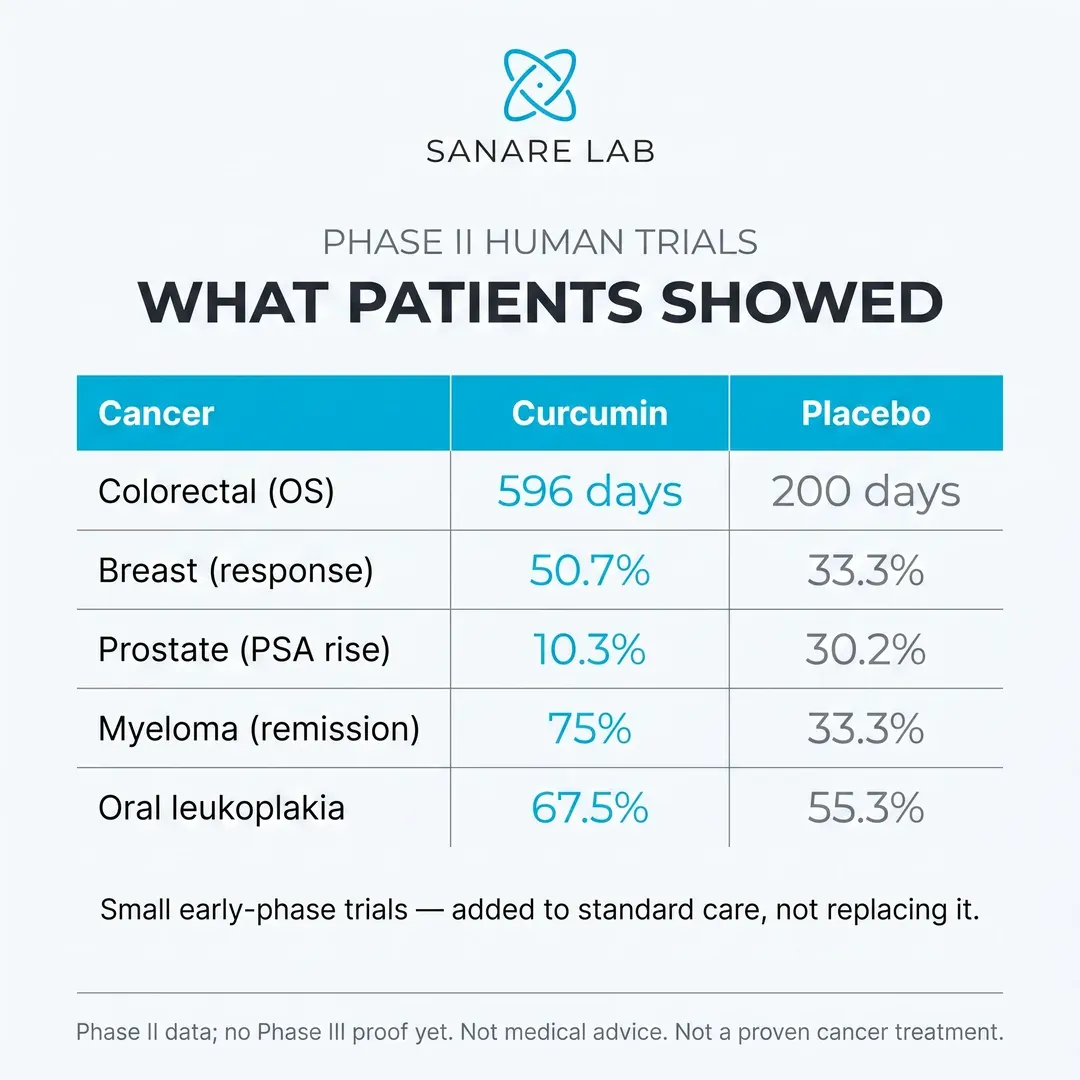
Important context: These are early-phase trials with relatively small sample sizes. For more details, see our guide on curcumin cancer mechanisms. The evidence is promising but not yet conclusive for any cancer type. Larger Phase III trials are needed to confirm these findings. Different curcumin formulations, dosages, and administration routes make direct comparisons difficult.
Curcumin + chemotherapy: synergy data
One of the most active areas of curcumin research is its potential to enhance the effectiveness of standard chemotherapy while reducing side effects. A comprehensive review in Molecules documented synergistic effects across multiple drug combinations:
A 2024 study in Nature Scientific Reports showed that curcumin synergistically enhanced gemcitabine efficacy against gemcitabine-resistant bile duct cancer cells by targeting the LAT2/glutamine pathway. In xenograft mouse models, the combination treatment produced the lowest tumor growth rate of all groups tested.
Notably, curcumin also appears to reduce the side effects of chemotherapy. The combination of curcumin and doxorubicin suppressed the reduction of glutathione peroxidase activity and decreased lipid peroxide levels in the heart — suggesting potential cardioprotective effects during chemotherapy.
Curcumin and immunotherapy
Emerging research has also explored combining curcumin with modern immunotherapy agents. Recent data showed that bisdemethoxycurcumin (BDMC), a curcumin derivative:
- Increased levels of tumor-infiltrating CD8+ T cells
- Enhanced IFN-γ secretion in the blood
- Decreased the number of tumor-infiltrating MDSCs (immune-suppressive cells)
- When combined with anti-PD-L1 antibodies, further enhanced secretion of IFN-γ, granzyme B, and perforin from CD8+ T cells
This is particularly relevant given the growing importance of immune checkpoint inhibitors in cancer treatment. For more details, see our guide on methylene blue in cancer research. Curcumin's ability to modulate the tumor microenvironment may make it a useful adjunct to PD-1/PD-L1 therapy.
Oral cancer: a Phase II breakthrough
One of the most promising clinical programs for curcumin is in oral cancer. Led by Dr. Marilene B. Wang at UCLA, a Phase II trial is investigating APG-157, a full-spectrum turmeric pastille, in patients with oral and oropharyngeal cancers.
The preceding Phase I trial confirmed:
- Safety and tolerability of the turmeric pastille
- Significant reduction of inflammatory cytokines in saliva
- Decreased tumor-associated microbes
- Recruitment of T-cells to the tumor microenvironment
APG-157 is expected to induce apoptosis in tumor cells, thereby reducing tumor burden and enhancing outcomes from subsequent local therapy. The Phase II trial is evaluating pathological responses, immune response biomarkers, and changes within tumor tissue.
Curcumin and Cancer Stem Cells
One of the most persistent problems in oncology is the cancer stem cell (CSC) — a small subpopulation of tumor cells with the ability to self-renew, differentiate, and regenerate an entire tumor after treatment. CSCs are widely believed to drive tumor initiation, metastasis, therapy resistance, and relapse, which is why conventional chemotherapy and radiation, effective at shrinking the bulk of a tumor, often fail to prevent recurrence: they leave the stem-like fraction behind.
Curcumin has attracted research attention precisely because preclinical studies suggest it can target several of the signaling pathways that keep cancer stem cells alive and self-renewing. The three developmental pathways most frequently implicated are Wnt/β-catenin, Notch, and Hedgehog — all of which are frequently hijacked by CSCs to maintain their undifferentiated, treatment-resistant state.
Wnt/β-catenin, Notch and Hedgehog signaling
In laboratory models, curcumin has been reported to suppress Wnt/β-catenin signaling by reducing nuclear accumulation of β-catenin and downregulating downstream targets such as cyclin D1 and c-Myc. It has also been shown to interfere with Notch signaling, another pathway essential for stem cell maintenance, and to modulate Hedgehog signaling in certain tumor types. A review of curcumin's effects on cancer stem cells summarized evidence across breast, colorectal, pancreatic, brain, and head and neck models, concluding that curcumin can reduce CSC markers (such as CD44 and ALDH1) and impair the sphere-forming capacity that is a hallmark of stem-like behavior (PMID 24463298).
More recent work has focused on triple-negative breast cancer (TNBC), an aggressive subtype with limited targeted options. A 2024 study in International Journal of Molecular Sciences found that curcumin and related polyphenol derivatives inhibited cancer stem-like cells in MDA-MB-231 TNBC cells, reducing their self-renewal capacity and stem cell marker expression (PMID 39000554). It is important to stress that these findings come from cell and animal models; no human trial has yet demonstrated that curcumin eradicates cancer stem cells in patients. Nevertheless, the CSC-targeting hypothesis is one of the more scientifically interesting rationales for continued research into curcumin as an adjunct rather than a standalone therapy.
Epigenetic Effects: How Curcumin May Reprogram Gene Expression
Beyond directly switching signaling pathways on or off, curcumin appears to act at the epigenetic level — influencing which genes are expressed without changing the underlying DNA sequence. Epigenetic dysregulation is now recognized as a fundamental driver of cancer, and because these modifications are potentially reversible, they represent an attractive therapeutic target.
DNA methylation and histone modification
Curcumin has been described in laboratory studies as a modulator of DNA methyltransferases (DNMTs), the enzymes responsible for adding methyl groups to DNA and silencing genes. By inhibiting DNMT activity, curcumin may help restore the expression of tumor suppressor genes that cancer cells have switched off through hypermethylation. Curcumin has also been reported to influence histone acetylation by modulating histone deacetylases (HDACs) and histone acetyltransferases (HATs), thereby altering how tightly DNA is packaged and how accessible genes are for transcription. These epigenetic mechanisms have been discussed extensively in the context of colorectal cancer, where curcumin's multi-target activity has been reviewed in detail (PMID 32088363).
MicroRNA regulation
A third layer of epigenetic control involves microRNAs (miRNAs) — small non-coding RNA molecules that fine-tune gene expression. Curcumin has been reported to restore the balance of tumor-suppressive and oncogenic miRNAs in various cancer models, for example by upregulating miR-34a and downregulating miR-21. A 2025 review in Frontiers in Pharmacology examined curcumin's regulation of microRNA networks across multiple malignancies, highlighting its potential to influence proliferation, apoptosis, and metastasis through miRNA modulation (Frontiers in Pharmacology, 2025). As with the other mechanisms discussed here, the evidence is predominantly preclinical, but it helps explain why curcumin exerts effects across such a broad range of cancer types.
Endoplasmic Reticulum Stress, Autophagy and Apoptosis
Curcumin's ability to trigger cancer cell death is not limited to classical apoptosis. Research has increasingly focused on how it manipulates two additional stress-response systems inside the cell: endoplasmic reticulum (ER) stress and autophagy. Understanding these mechanisms helps explain why curcumin can kill cancer cells that have become resistant to conventional apoptosis-inducing drugs.
The endoplasmic reticulum is the cellular compartment responsible for folding and processing proteins. When it becomes overwhelmed — a state called ER stress — the cell activates the unfolded protein response (UPR). Mild ER stress promotes survival, but severe or prolonged ER stress flips the switch toward programmed cell death. In ovarian, hepatic, and glioma cell models, curcumin has been shown to induce excessive ER stress and reactive oxygen species, tipping cancer cells past the point of no return and into apoptosis.
Autophagy: friend or foe
Autophagy is the process by which cells recycle their own damaged components. In cancer, autophagy is a double-edged sword: it can protect stressed tumor cells and help them survive chemotherapy, or, when pushed to extremes, it can drive a form of cell death known as autophagic cell death. Curcumin has been reported to modulate autophagy in a context-dependent manner. In colorectal cancer specifically, a 2024 review in Phytotherapy Research detailed how curcumin regulates autophagy through pathways including AMPK/mTOR signaling, and how this interacts with its pro-apoptotic effects (PMID 38699926).
In ovarian cancer models, curcumin has been shown to induce mitochondrial dysfunction and oxidative DNA damage, further linking its pro-oxidant activity within cancer cells to cell death (PMID 40163489). This is an important nuance: while curcumin behaves as an antioxidant in healthy tissue at normal doses, inside cancer cells under certain conditions it can act as a pro-oxidant, generating the reactive oxygen species that overwhelm the cell's defenses.
Additional Cancer Types: Ovarian, Cervical, Gastric, Bladder and Melanoma
While the human clinical evidence is concentrated in a handful of cancers (breast, colorectal, prostate, pancreatic, and oral), preclinical research has explored curcumin across a much wider range of malignancies. The table below summarizes representative findings in cancers less commonly discussed. As with all preclinical data, these results describe activity in cells and animals — not proven clinical benefit in patients.
The ovarian findings are among the most recent and mechanistically interesting. A 2025 study in Medical Oncology demonstrated that curcumin suppressed malignant behaviors of ovarian cancer by regulating tumor-associated macrophages, shifting them away from the immunosuppressive M2 phenotype (PMID 40185946). Broader reviews of curcumin activity across gastric, bladder, melanoma, and renal cancers describe consistent modulation of Wnt, PI3K/Akt, and STAT3 signaling (IntechOpen, 2024), while hematologic malignancy models point to apoptosis induction in AML and lymphoma (PMC10927384).

Curcumin Turmeric 360 mg per Serving — with Black Pepper & Phytosome Extract | Joint & Cellular Support | 120 Capsules
Curcumin and Radiation Therapy: Radiosensitization and Radioprotection
One of the more clinically relevant areas of curcumin research is its dual relationship with radiation therapy. In principle, curcumin may help on both sides of the equation: making cancer cells more vulnerable to radiation (radiosensitization) while helping protect healthy tissue from radiation-induced side effects (radioprotection). This apparent paradox — sensitizing tumor cells while protecting normal cells — is one of the most attractive features of curcumin as a potential adjunct.
Radiosensitization of tumor cells
Radiation kills cancer cells largely by generating DNA damage and reactive oxygen species, but tumor cells frequently upregulate survival pathways (particularly NF-κB) to resist this damage. Because curcumin suppresses NF-κB and related survival signaling, preclinical studies suggest it can lower the threshold at which cancer cells succumb to radiation. Laboratory and animal research has reported enhanced radiation-induced cell death across several tumor types when curcumin is added, supporting the concept of curcumin as a radiosensitizer (PMC8869399).
Radioprotection of healthy tissue
On the protective side, the most robust human evidence concerns radiation-induced oral mucositis — the painful inflammation of the mouth and throat lining that affects most head and neck cancer patients undergoing radiotherapy. A 2025 meta-analysis in Frontiers in Pharmacology found that curcumin, across several pharmaceutical forms, significantly reduced the severity and incidence of oral mucositis during cancer treatment (PMID 40242451). A separate 2024 systematic review reached a similar conclusion regarding curcumin's role in mitigating radiotherapy-associated mucositis (European Journal of Clinical Pharmacology, 2024). This is one of the few areas where curcumin has moved beyond theoretical benefit into demonstrable, patient-relevant outcomes — although the benefit is supportive (reducing side effects) rather than anti-cancer per se.
Curcumin Analogs: EF24, BDMC and the Next Generation
Curcumin's greatest weakness as a drug is its poor bioavailability and rapid metabolism. To overcome this, medicinal chemists have designed synthetic analogs — molecules structurally based on curcumin but engineered for greater potency and stability. These next-generation compounds are an active area of preclinical drug development.
EF24: a more potent synthetic analog
EF24 (a diphenyl difluoroketone) is the most extensively studied curcumin analog and is generally reported to be 10 to 20 times more potent than natural curcumin in laboratory assays. It retains curcumin's core mechanisms — NF-κB and MAPK inhibition — but with dramatically improved cellular activity. EF24 has been shown to trigger p38 MAPK-mediated apoptosis in cancer cells (PMID 32759757), to suppress hepatocellular carcinoma in vivo and in vitro (PMID 23118928), and to inhibit proliferation and invasion of triple-negative breast cancer cells (PMID 34780286). A liposomal formulation, Lipo-EF24, has been developed to improve delivery and has shown activity against pancreatic cancer in preclinical models (PMID 27401816).
Bisdemethoxycurcumin and other curcuminoids
Natural turmeric contains a family of related curcuminoids beyond curcumin itself, including demethoxycurcumin (DMC) and bisdemethoxycurcumin (BDMC). BDMC in particular has attracted interest for its relatively greater metabolic stability and its documented effects on immune signaling and PD-L1 regulation in preclinical models. These curcuminoids, along with fully synthetic analogs, illustrate an important point for consumers: the "curcumin" studied in a given paper is not always identical to the compound in a given supplement. This is one more reason why standardized, well-characterized formulations matter when translating research into practice.
Nanoparticle Delivery: Closing the Bioavailability Gap
If poor absorption is curcumin's central limitation, then delivery technology is where the field is advancing most rapidly. Beyond the phytosome and piperine approaches discussed earlier, a wave of nanoparticle and molecular-encapsulation strategies has emerged, some reporting dramatic increases in bioavailability in preclinical and early clinical testing.
A 2026 review of curcumin nanoparticle delivery systems reported bioavailability improvements of up to 178-fold with advanced formulations and noted that more than 210 clinical trials have now investigated curcumin in various forms (PMC12894192). Other recent delivery innovations include gamma-cyclodextrin metal-organic frameworks (γ-CD-MOF) reporting up to 267-fold improvements (PMC11665533), and ascorbic acid cocrystals and chitosan-based systems reporting even larger gains in specific assays (AAPS PharmSciTech, 2025). Milk-derived exosomes have also been explored as natural nanocarriers for curcumin delivery (PMID 38452655).
The practical takeaway is unchanged but reinforced: the form of curcumin you take determines whether meaningful amounts reach your bloodstream at all. For most consumers, a well-formulated phytosome-based curcumin with black pepper extract represents the best-researched, commercially available balance of absorption and value, while the exotic nanoparticle systems remain largely confined to the laboratory for now.
What the Meta-Analyses Actually Conclude (2024–2026)
Individual studies can be cherry-picked to support almost any position, which is why systematic reviews and meta-analyses — which pool data across many trials — are the most reliable guide to what curcumin does and does not do in humans. The honest summary of the most recent evidence is nuanced, and worth stating plainly.
A 2025 systematic review examining curcumin as an adjunct in cancer treatment found no consistent evidence that curcumin improves overall survival or progression-free survival in cancer patients (PMC10144810). In other words, despite thousands of promising laboratory studies, curcumin has not been shown to make people with cancer live longer. This is the single most important fact for any consumer to understand.
Where meta-analyses are more encouraging is in supportive care and safety. Pooled analyses consistently confirm that curcumin is remarkably well tolerated even at high doses, and that it can reduce specific treatment-related side effects — most notably radiotherapy-induced oral mucositis (PMID 40242451). A large 2024 evidence synthesis reviewing hundreds of studies likewise emphasized curcumin's favorable safety profile and its potential as a complementary agent, while cautioning that high-quality clinical efficacy data remain limited (Naunyn-Schmiedeberg's Archives of Pharmacology, 2024). The consensus, then, is that curcumin is best understood today as a well-tolerated supportive and investigational agent — not a proven treatment.
Safety Profile and Drug Interactions
Curcumin's safety record is one of its strongest attributes and a major reason for its enduring research interest. Human trials have administered oral curcumin at doses as high as 8 grams per day for several months in a Phase I trial without dose-limiting toxicity (PMID 11712783), and a dose-escalation study reported that single doses up to 12 grams were well tolerated, with only mild gastrointestinal effects (PMID 16545122). The most common side effects at high doses are mild: nausea, diarrhea, and a yellow discoloration of the stool.
Two caveats deserve emphasis. First, rare cases of liver injury have been reported, most often linked to high-dose products or to adulterated supplements, sometimes containing undeclared piperine at levels that alter drug metabolism. Second, curcumin is not inert with respect to prescription medication. It can interact with the cytochrome P450 enzyme system — particularly CYP3A4 and CYP2D6 — and with drug transporters, potentially altering the blood levels of a range of medications. The table below summarizes the most clinically relevant interaction categories.
Because piperine (black pepper extract) is added to many curcumin formulations specifically to boost absorption, it is worth noting that piperine itself inhibits certain drug-metabolizing enzymes. This is beneficial for curcumin uptake but is exactly why anyone taking prescription medication — and especially anyone undergoing cancer treatment — should discuss curcumin supplementation with their oncologist or pharmacist before starting. The U.S. National Cancer Institute maintains a detailed summary of curcumin's pharmacology, safety, and interactions in its curcumin PDQ resource (NCI, curcumin PDQ).
Curcumin and Fenbendazole: What the Evidence Actually Shows
A frequent question — driven largely by online anecdotes — is whether curcumin should be combined with fenbendazole, an anti-parasitic drug that has attracted attention in alternative cancer communities. It is essential to address this honestly and without overstatement.
There is currently zero direct scientific evidence — no human trials and no controlled preclinical studies — evaluating the specific combination of curcumin and fenbendazole for cancer. Any claim that these two compounds work synergistically against cancer is not supported by published research. The association between them comes almost entirely from a single widely-shared personal anecdote: the Joe Tippens protocol, in which an individual with advanced lung cancer reported taking fenbendazole alongside curcumin, vitamin E, and CBD oil. This is an uncontrolled, single-person account with multiple simultaneous variables — it cannot establish that either compound, let alone the combination, was responsible for any outcome.
The scientific interest in fenbendazole itself rests on preclinical observations of microtubule disruption and metabolic effects, but a widely-cited review has emphasized that robust clinical evidence for fenbendazole as a cancer treatment does not yet exist (Anticancer Research, 2024). Readers interested in the underlying pharmacology can review our detailed comparison of fenbendazole versus mebendazole. The responsible position is this: curcumin has a substantial and growing body of mechanistic research behind it, whereas the curcumin–fenbendazole combination remains purely anecdotal. Anyone considering such a combination should do so only under medical supervision and with a clear understanding that it is experimental and unproven.
✅ What this means for informed consumers
From a scientific perspective, the current evidence supports understanding curcumin as:
- A biologically active polyphenol with well-documented molecular effects across at least 7 cancer types
- A compound where formulation quality matters far more than raw dose — phytosome and nanoparticle forms are 9–130× more bioavailable than raw powder
- A promising adjunct to chemotherapy with synergistic effects documented for 5-FU, cisplatin, doxorubicin, docetaxel, gemcitabine, and paclitaxel
- A compound with a favorable safety profile — safe at doses up to 12 g/day in Phase I trials, and associated with fewer adverse events than placebo in at least one large RCT
- An ingredient whose clinical evidence is encouraging but still preliminary — larger Phase III trials are needed
Modern research does not support simplistic claims, but it does justify continued interest in high-quality, bioavailable curcumin formulations as part of evidence-informed wellness strategies.
Bottom line
Curcumin is one of the most extensively studied natural compounds in cancer-related research. While it is not a standalone cancer treatment, the clinical trial data is increasingly compelling: median survival tripled in a colorectal cancer trial, objective response rates nearly doubled in breast cancer when combined with paclitaxel, and PSA progression was reduced threefold in prostate cancer.
The field has moved well beyond "lab-only" findings. With multiple Phase II trials complete and more underway, understanding the difference between raw turmeric, standardized extracts, and advanced delivery systems is more important than ever.
Frequently Asked Questions
Does curcumin cure cancer?
Answer: No. There is no credible scientific evidence that curcumin cures cancer in humans. Meta-analyses have found no consistent improvement in overall survival or progression-free survival among cancer patients taking curcumin. It is best understood as a well-tolerated investigational and supportive agent that is actively researched — not a treatment or cure.
What is the difference between turmeric, curcumin, and curcuminoids?
Answer: Turmeric is the root spice; it contains only about 2–5% curcuminoids by weight. Curcuminoids are the family of active compounds in turmeric, of which curcumin is the most abundant and studied (alongside demethoxycurcumin and bisdemethoxycurcumin). Most research uses standardized curcumin extracts, not raw turmeric powder, which is far too dilute to reach studied doses.
Why is bioavailability such a big issue with curcumin?
Answer: Plain curcumin is poorly absorbed, rapidly metabolized, and quickly eliminated, so very little reaches the bloodstream. This is why formulation matters enormously and why raw turmeric or cheap curcumin capsules may deliver negligible systemic levels.
Which curcumin formulation is best absorbed?
Answer: Phytosome (phospholipid-bound) curcumin and formulations combining curcumin with piperine (black pepper extract) are the best-researched, commercially available options for improved absorption. Newer nanoparticle systems report even higher bioavailability in the lab, but remain largely experimental. For most consumers, a standardized phytosome curcumin with black pepper extract offers the best evidence-based balance.
How much curcumin is safe to take?
Answer: Human trials have used oral doses up to 8 grams per day for months without dose-limiting toxicity, and single doses up to 12 grams have been tolerated. That said, most supplements are dosed far lower, and more is not necessarily better. Anyone on medication or in cancer treatment should confirm an appropriate dose with their doctor.
What are the side effects of curcumin?
Answer: At high doses the most common effects are mild gastrointestinal symptoms — nausea, diarrhea, and yellow-colored stool. Rare cases of liver injury have been reported, most often linked to high-dose or adulterated products. Overall, curcumin has an excellent safety profile.
Can I take curcumin during chemotherapy?
Answer: This must be decided with your oncologist. Curcumin can affect drug-metabolizing enzymes (CYP3A4, CYP2D6) and may alter chemotherapy blood levels, and there is ongoing debate about whether its antioxidant activity could interfere with certain treatments. Never add curcumin to an active cancer regimen without medical guidance.
Does curcumin interact with blood thinners?
Answer: Yes, potentially. Curcumin has mild antiplatelet activity and may increase bleeding risk when combined with anticoagulants or antiplatelet drugs such as warfarin, aspirin, or clopidogrel. Discuss this with your prescriber, especially before surgery.
Does curcumin work better with black pepper?
Answer: Piperine, the active compound in black pepper, can significantly increase curcumin absorption by slowing its metabolism. This is why many formulations include it. The same enzyme inhibition that helps curcumin, however, can also affect other medications — another reason to review your full medication list with a pharmacist.
Is IV curcumin more effective than oral curcumin?
Answer: Intravenous delivery bypasses the absorption problem and achieves far higher blood levels. In one randomized trial, IV curcumin combined with paclitaxel produced a higher response rate than paclitaxel alone in metastatic breast cancer, whereas an oral curcumin-plus-docetaxel study failed — illustrating that delivery route matters. IV curcumin is only appropriate in a clinical setting and is not a substitute for standard care.
Which cancers has curcumin been studied in most?
Answer: Human clinical data are most developed in colorectal, breast, prostate, pancreatic, and oral cancers. Preclinical research extends much further — to ovarian, cervical, gastric, bladder, melanoma, and hematologic cancers — but those findings remain at the cell and animal stage.
What are curcumin analogs like EF24?
Answer: EF24 is a synthetic molecule based on curcumin's structure, engineered to be roughly 10–20 times more potent with better stability. It is a promising preclinical drug candidate — studied in pancreatic, liver, and triple-negative breast cancer models — but it is not a dietary supplement and is not available to consumers.
Can curcumin help with radiation therapy side effects?
Answer: This is one of the strongest areas of human evidence. Multiple meta-analyses show curcumin reduces the severity and incidence of radiation-induced oral mucositis. Separately, preclinical work suggests it may sensitize tumor cells to radiation, though that anti-cancer effect is not yet proven in patients.
Should I combine curcumin with fenbendazole?
Answer: There is no scientific evidence — no human trials and no controlled studies — supporting the curcumin–fenbendazole combination for cancer. The association comes from a single personal anecdote (the Joe Tippens story), not research. If you are considering it, do so only under medical supervision and with the understanding that it is unproven and experimental.
Does curcumin affect cancer stem cells?
Answer: In laboratory models, curcumin has been reported to suppress cancer stem cell pathways such as Wnt/β-catenin and Notch and to reduce stem cell markers. This is scientifically interesting because cancer stem cells drive relapse, but it has not been demonstrated in human patients.
Can healthy people take curcumin to prevent cancer?
Answer: There is no proof that curcumin prevents cancer in humans. It is widely used as a general wellness and anti-inflammatory supplement with a strong safety record, but "prevention" claims go beyond the current evidence. Treat it as a supportive supplement, not a preventive medicine.
Does curcumin kill cancer cells?
Answer: In laboratory studies, curcumin has demonstrated the ability to induce apoptosis (programmed cell death) in multiple cancer cell lines, including breast, colorectal, prostate, lung, and pancreatic. However, killing cancer cells in a petri dish is not the same as treating cancer in a living person. Human clinical trials have shown modest biomarker improvements, but no Phase III trial has yet proven that curcumin alone can eliminate tumors. It remains a promising adjunct under active investigation, not a standalone cure.
What is the best curcumin dosage for cancer?
Answer: Clinical trials have used doses ranging from 500 mg to 8,000 mg of standardized curcumin per day, with most oncology-focused studies using 1,000–2,000 mg/day of a bioavailability-enhanced formulation (such as Curcumin C3 Complex with piperine, or Meriva phytosome). There is no universally agreed-upon "cancer dose." The Joe Tippens Protocol specifies 600 mg/day of bioavailable curcumin. Doses above 8,000 mg/day have been associated with gastrointestinal side effects. Always consult a physician before choosing a dose, especially if you are on chemotherapy or blood thinners.
Curcumin vs turmeric — what is the difference for cancer?
Answer: Turmeric is the whole spice (Curcuma longa root), while curcumin is the most active polyphenol extracted from it. Raw turmeric powder contains only about 2–5% curcuminoids by weight. Clinical cancer studies use standardized curcumin extracts at doses (500–8,000 mg/day) that would be impossible to achieve from dietary turmeric alone. For any pharmacological effect relevant to oncology, a concentrated curcumin supplement — ideally with enhanced bioavailability — is required, not turmeric powder.
What do clinical trials say about curcumin and cancer?
Answer: As of 2026, over 50 clinical trials have evaluated curcumin in cancer patients. Key findings include: curcumin + FOLFOX improved response rates in metastatic colorectal cancer (2012, Phase II); curcumin lozenges reduced oral precancerous lesion size in a Phase II trial; and curcumin + gemcitabine showed a trend toward improved survival in pancreatic cancer. However, many trials are small (under 50 patients), and no large Phase III trial has confirmed curcumin as a standard cancer therapy. The evidence supports curcumin as a well-tolerated adjunct worthy of further study.
Is Curcumin C3 Complex better for cancer than other forms?
Answer: Curcumin C3 Complex is the most clinically studied curcumin extract, used in over 65 published human trials. It contains a standardized ratio of curcumin (~77%), demethoxycurcumin (~17%), and bisdemethoxycurcumin (~3%). Other forms like Meriva (phytosome) and Theracurmin (nanoparticle) achieve higher blood levels per milligram, but C3 Complex has the largest safety and efficacy dataset. The "best" form depends on the clinical context: C3 Complex for evidence depth, phytosome formulations for higher plasma curcumin levels at lower doses. No head-to-head cancer outcome trial has compared them.
Shop Sanare Lab
Lab-tested products referenced in the research above. Links are provided for convenience — always review the label and consult a professional before use.
120 capsules — with Black Pepper for absorption
180 capsules — 99% purity, laboratory tested
6 / 12 / 18 mg — 100 tablets
Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.
References
- Giordano A, Tommonaro G. Curcumin and cancer. Nutrients, 2019. PMID: 31412624. PubMed
- Kunnumakkara AB, Bordoloi D, Padmavathi G et al.. Curcumin, the golden nutraceutical: multitargeting for multiple chronic diseases. Br J Pharmacol, 2017. PMID: 27638428. PubMed
- Tomeh MA, Hadianamrei R, Zhao X. A review of curcumin and its derivatives as anticancer agents. Int J Mol Sci, 2019. PMID: 31060180. PubMed
- Dhillon N, Aggarwal BB, Newman RA et al.. Phase II trial of curcumin in patients with advanced pancreatic cancer. Clin Cancer Res, 2008. PMID: 18594006. PubMed
- Bayet-Robert M, Kwiatkowski F, Leheurteur M et al.. Phase I dose escalation trial of docetaxel plus curcumin in patients with advanced and metastatic breast cancer. Cancer Biol Ther, 2010. PMID: 20087030. PubMed
- Anand P, Kunnumakkara AB, Newman RA, Aggarwal BB. Bioavailability of curcumin: problems and promises. Mol Pharm, 2007. PMID: 17999464. PubMed
- Shoba G, Joy D, Joseph T et al.. Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers. Planta Med, 1998. PMID: 9619120. PubMed
- Aggarwal BB, Kumar A, Bharti AC. Anticancer potential of curcumin: preclinical and clinical studies. Anticancer Res, 2003. PMID: 12680238. PubMed
- Devassy JG, Nwachukwu ID, Jones PJ. Curcumin and cancer: barriers to obtaining a health claim. Nutr Rev, 2015. PMID: 26024546. PubMed
- Carroll RE, Benya RV, Turgeon DK et al.. Phase IIa clinical trial of curcumin for the prevention of colorectal neoplasia. Cancer Prev Res, 2011. PMID: 21372035. PubMed
- Hewlings SJ, Kalman DS. Curcumin: a review of its effects on human health. Foods, 2017. PMID: 29065496. PubMed
- Gupta SC, Patchva S, Aggarwal BB. Therapeutic roles of curcumin: lessons learned from clinical trials. AAPS J, 2013. PMID: 23054972. PubMed
- Maheshwari RK, Singh AK, Gaddipati J, Srimal RC. Multiple biological activities of curcumin: a short review. Life Sci, 2006. PMID: 16413584. PubMed
- Sordillo LA, Sordillo PP. Targeting cancer stem cells by curcumin and clinical applications. Cancer Lett, 2014. PMID: 24463298. PubMed
- Inhibition of cancer stem-like cells by curcumin and other polyphenol derivatives in MDA-MB-231 TNBC cells. Int J Mol Sci, 2024. PMID: 39000554. PubMed
- Weng W, Goel A. Curcumin and colorectal cancer: an update and current perspective on this natural medicine. Semin Cancer Biol, 2022. PMID: 32088363. PubMed
- Curcumin regulation of microRNA networks in cancer: mechanisms and therapeutic potential. Front Pharmacol, 2025. Frontiers in Pharmacology
- Curcumin and its anti-colorectal cancer potential: from mechanisms of action to autophagy. Phytother Res, 2024. PMID: 38699926. PubMed
- Curcumin induces mitochondrial dysfunction-associated oxidative DNA damage in ovarian cancer cells. PLoS One, 2025. PMID: 40163489. PubMed
- Curcumin suppresses malignant behaviors of ovarian cancer through regulation of tumor-associated macrophages. Med Oncol, 2025. PMID: 40185946. PubMed
- Curcumin in gastric, bladder, melanoma and renal cancers: modulation of Wnt, PI3K/Akt and STAT3 signaling. IntechOpen, 2024. IntechOpen
- Curcumin in hematologic malignancies: apoptosis induction in acute myeloid leukemia and lymphoma models. PMC, 2024. PMC10927384
- Curcumin as a radiosensitizer: preclinical evidence across tumor types. PMC, 2022. PMC8869399
- Curcumin for the prevention and management of radiotherapy-induced oral mucositis: a systematic review. Eur J Clin Pharmacol, 2024. Springer
- Efficacy of different pharmaceutical forms of Curcuma longa or curcumin in reducing oral mucositis severity and incidence: a meta-analysis. Front Pharmacol, 2025. PMID: 40242451. PubMed
- The curcumin analogue EF-24 triggers p38 MAPK-mediated apoptotic cell death. Cancers, 2020. PMID: 32759757. PubMed
- In vivo and in vitro suppression of hepatocellular carcinoma by EF24, a curcumin analog. PLoS One, 2012. PMID: 23118928. PubMed
- The curcumin analog EF24 inhibits proliferation and invasion of triple-negative breast cancer cells. Mol Cell Biol, 2022. PMID: 34780286. PubMed
- A liposomal formulation of the synthetic curcumin analog EF24 (Lipo-EF24) inhibits pancreatic cancer progression. J Nanobiotechnology, 2016. PMID: 27401816. PubMed
- Curcumin nanoparticle delivery systems: advances in bioavailability and clinical translation. PMC, 2026. PMC12894192
- Gamma-cyclodextrin metal-organic framework for enhanced curcumin bioavailability. PMC, 2024. PMC11665533
- Curcumin cocrystal and chitosan-based delivery systems for improved oral bioavailability. AAPS PharmSciTech, 2025. Springer
- Curcumin encapsulated in milk small extracellular vesicles as a nanotherapeutic alternative. Biomed Pharmacother, 2024. PMID: 38452655. PubMed
- Efficacy of curcumin as an adjunct in cancer treatment: a systematic review. PMC, 2025. PMC10144810
- Curcumin in cancer therapy: a comprehensive evidence synthesis of preclinical and clinical studies. Naunyn Schmiedebergs Arch Pharmacol, 2024. Springer
- Cheng AL, Hsu CH, Lin JK et al.. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res, 2001. PMID: 11712783. PubMed
- Lao CD, Ruffin MT, Normolle D et al.. Dose escalation of a curcuminoid formulation. BMC Complement Altern Med, 2006. PMID: 16545122. PubMed
- National Cancer Institute. Curcumin (PDQ): health professional version — pharmacology, safety and drug interactions. NCI, 2024. cancer.gov
- Fenbendazole as an anticancer agent: a critical appraisal of the evidence. Anticancer Res, 2024. Anticancer Research
frontiersin.org View the primary 2024 review article →
Protocol Stack (Quick Links)
Below are commonly referenced items mentioned in this article. Links are provided for convenience — always review the label and consult a professional before use.
Curcumin Turmeric
360 mg per capsule — 120 capsules with Black Pepper & Phytosome Extract Buy Curcumin Turmeric →Fenbendazole 222 mg
180 capsules — 99% purity, laboratory tested Buy Fenbendazole 222 →Blue Essence (Methylene Blue)
60 capsules with Vitamin C + Organic Cocoa Powder Buy Blue Essence →Disclaimer: Links are informational and for convenience. This site does not provide medical advice and does not endorse any specific vendor. Always verify product quality, labeling, and consult a licensed professional for health decisions.
Curcumin Absorption Maximizer Guide
Stop wasting money on curcumin that your body can't absorb. Get the complete guide to maximizing bioavailability — with specific product recommendations, timing protocols, and absorption-boosting combinations backed by clinical research.
Download Free Curcumin Absorption Maximizer Guide (PDF)
Medical Disclaimer
This article is for educational and informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.

Dr. Andrew Ellison, MD
Science editor and health researcher at Sanare Lab, covering evidence-based wellness, emerging compound research, clinical studies, and practical health protocols. Content is educational and does not replace medical advice.